We discussed an elderly woman with AML on palliative chemotherapy who presented with subacute neck swelling and acute fever, found to have neutropenic fever with tonsillitis.






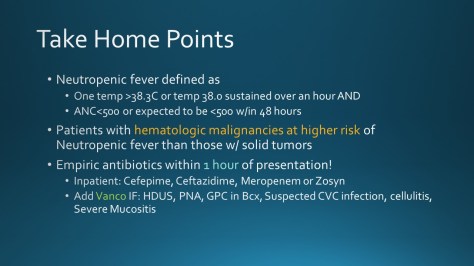

We discussed an elderly woman with AML on palliative chemotherapy who presented with subacute neck swelling and acute fever, found to have neutropenic fever with tonsillitis.
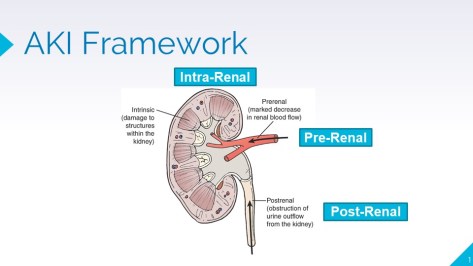
Today, we talked about a case of a elderly female who presented with lithium toxicity triggered by dehydration. In the process, we went over a framework for AKI and discussed why FENa & FEUrea are only used to distinguish between pre-renal and ATN



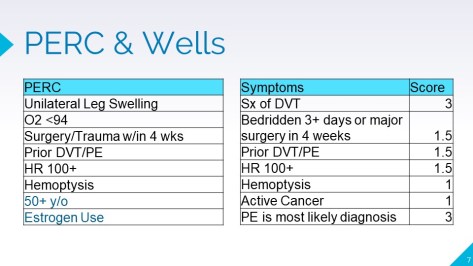
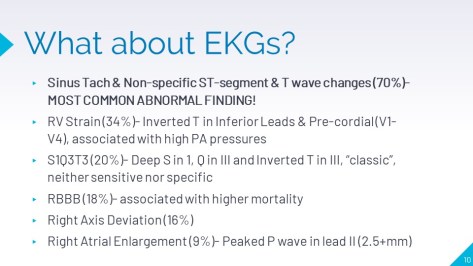
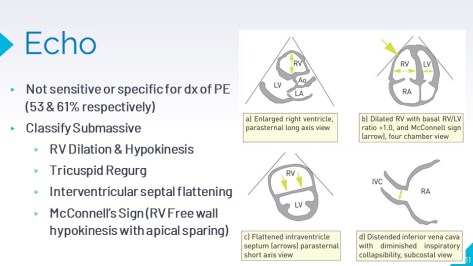
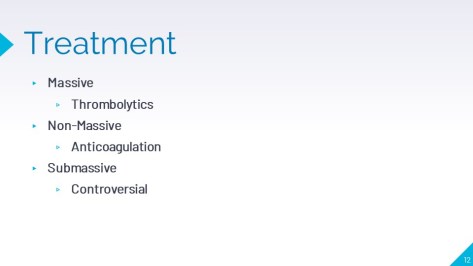
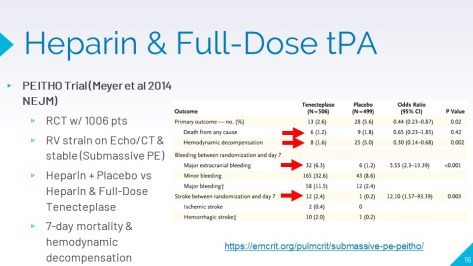
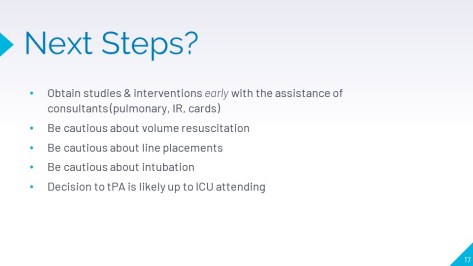
Today we had a 33y/o M with hx of obesity, HTN, IDDM2 who presented with acute SOB and found to have submassive PE




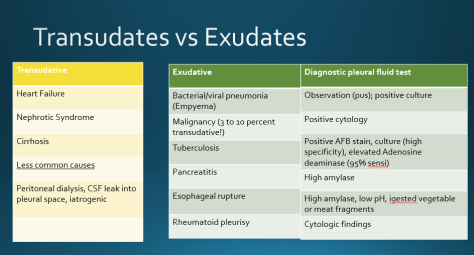
Today we discussed the case of an older man with alcohol use disorder with subacute-chronic cough, with recent 10-day course of amoxicillin for treatment of community acquired pneumonia, who was found to have unilateral pleural effusion found to be an empyema.





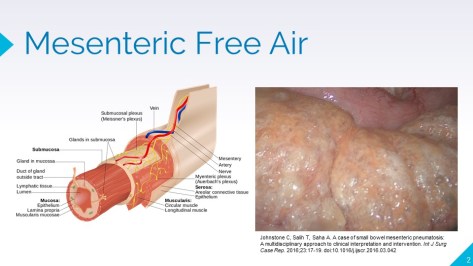
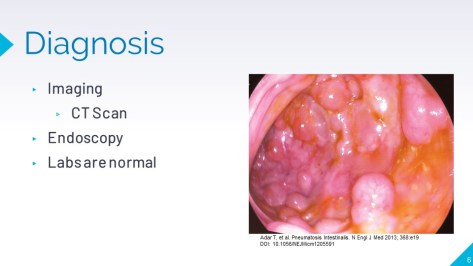
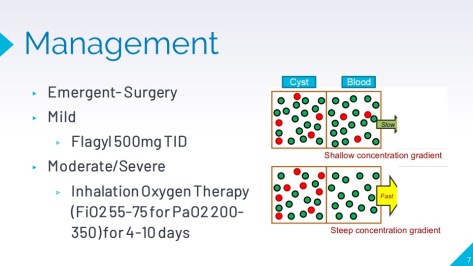
Today, we had a case of a middle aged female with hx of endometrial carcinoma on Pembrolizumab and Lenvatinib who presented with worsening diarrhea, PO intake, weight loss, and found to have pneumatosis intestinalis due to chemotherapy

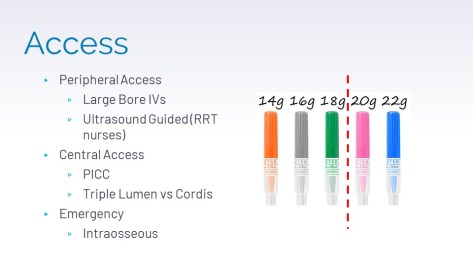
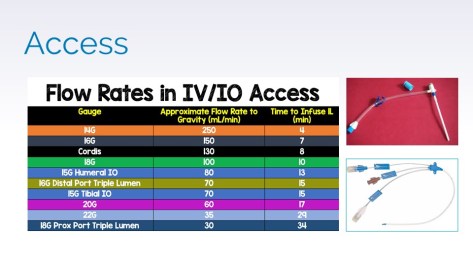
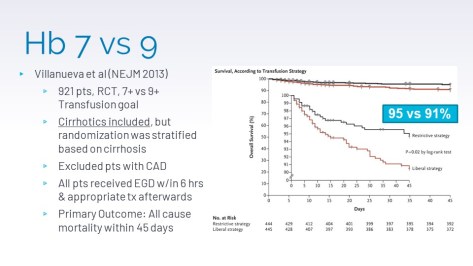
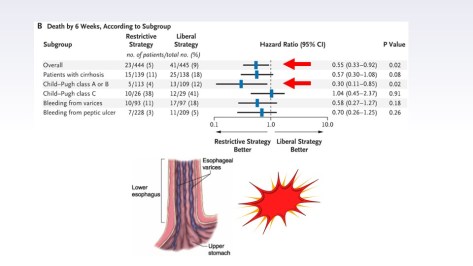
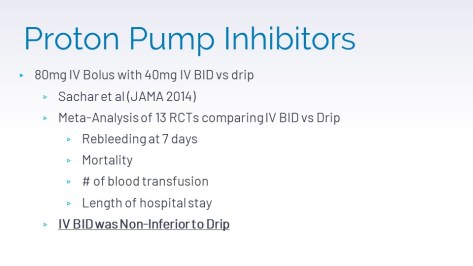
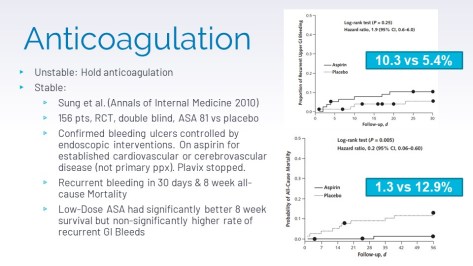
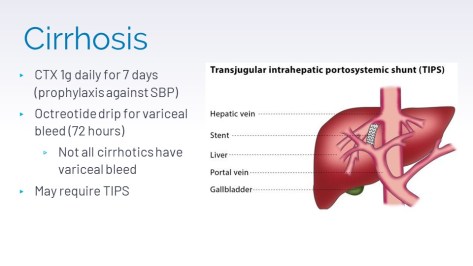
Today we had a case of a middle aged female presents with weeks of progressive SOB & fatigue and an episode of hematochezia, found to have a Hb of 3.4. This became a good case to discuss how to approach GI emergencies




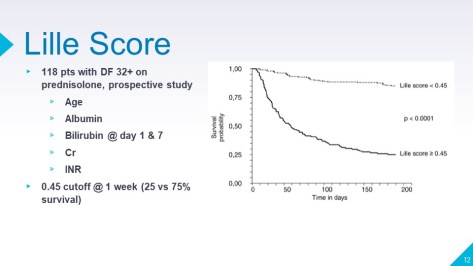
Today we had a case of a young female with a history of etoh abuse who presented with 1 week of RUQ ab pain, n/v poor PO intake and found to have alcoholic hepatitis.












Today, Dr. Nhat Pham took us through the pathophysiology for and evidence behind SGLT2 inhibitor use in our patients with nephropathy. Here is a review:
SGLT2 is a sodium/glucose cotransporter expressed in the proximal tubules of the kidney. Its function is to reabsorb sodium and glucose after they are filtered through the glomerulus. When we inhibit SGLT2 with these medications, it results in significant natriuresis, glucosuria, and associated osmotic diuresis. This lowers blood glucose by losing more serum glucose in the urine, but only modestly, resulting in Hemoglobin A1C reduction of only 0.5-0.8%. Three SGLT2 inhibitors are currently available in the United States: empagliflozin (Jardiance), canagliflozin (Invokana), and dapagliflozin (Farxiga).
Recent trials (EMPA-REG, CANVAS, CREDENCE, and DAPA-HF among others) have shown improvement in not only glycemic control, but also cardiovascular and renal outcomes above that which is expected from their effect on A1c. There are many theories on the mechanism by which these meds improve cardiovascular outcomes (improved afterload by changing vascular structure and function, improved cardiac metabolism via ketogenesis, inhibition of myocardial Na/H exchange, decrease in cardiac fibrosis and necrosis, and uric acid metabolism), but it is not clear what is actually driving this decrease in mortality. It is clear that something beyond just their diuretic effect is at play.
We went over the following 2 trials:
The CANVAS/CANVAS-R trials took over 10,000 patients with type 2 diabetes and known CAD or elevated risk of CAD and randomized them to receive high dose Canagliflozin (300mg) or placebo. The results showed a decrease in cardiovascular mortality, decrease in heart failure admissions, decreased nonfatal stroke, decreased nonfatal MIs, decreased progression to ESRD, and slower decline in GFR. Some adverse effects were highlighted in the trial including lower extremity amputation, mycotic genital infections, and volume depletion from osmotic diuresis.
The CREDENCE trial took over 4 thousand patients with DM2 and albuminuria and randomized them to lower dose Canagliflozin (100mg). These patients were already on ACEI/ARBs for at least 4 weeks prior to initiation of the trial. Canagliflozin was found to decrease the progression of GFR decline so significantly that it was stopped early due to clear benefit. This trial did not show an increase in lower extremity amputation risk.
In diabetes, chronically elevated serum glucose levels cause lots of glucose to be filtered through the glomerulus. This upregulates SGLT2 expression in the proximal tubule, causing it to reabsorb more and more glucose and sodium in a process called hyperfiltration. The macula densa then senses a low sodium concentration in the distal tubule, making it think the kidneys are being hypoperfused, and signals the afferent arterial to vasodilate. This causes increased pressure in the glomerulus due to increased blood flow, which over time causes scarring and nephron loss, eventually leading to a decrease in GFR.
SGLT2 inhibitors alter the physiology of diabetic nephropathy through a mechanism called tubuloglomerular feedback (or TG feedback for short). By inhibiting the upregulated reabsorption of glucose and sodium by SGLT2 in the proximal tubule, we increase the amount of sodium that the macula densa senses in the distal tubule. It no longer thinks the kidneys are hypoperfused, but thinks that they are getting too much blood flow and signals the afferent arteriole to vasoconstrict. This decreases the pressure in the glomerulus, preventing some of the scarring and nephron loss that occurs with hyperfiltration.
ACEI/ARBs are the mainstay of therapy for diabetic nephropathy and have a robust body of evidence supporting their use to prevent progression to ESRD. They work by decreasing glomerular pressure via dilating the efferent arteriole. All of our patients with diabetic nephropathy should be on ACEI/ARBs if they can tolerate them. The effects of SGLT2 inhibitors are thought to be synergistic, as evidenced by the added renal benefit of SGLT2 inhibitors in patients already on ACEI/ARBs.
The data is still emerging on SGLT2 inhibitors and more studies are necessary to fully understand how we should look at each of these adverse effects, but some are widely accepted. These medications do cause a significant diuretic effect and do require a reduction in baseline diuretic regimen upon initiation to avoid overdiuresis. In addition, there is an initial reduction in GFR (or AKI) that is to be expected from the reduction in glomerular pressure from vasoconstriction of the afferent arteriole. Dr. Pham considers an increase in Cr of 20% or less acceptable. An increase in the incidence of mycotic genital infections is also an accepted consequence of thees medications.
The FDA has a boxed warning about SGLT2 inhibitors’ increase in risk of lower limb amputation, which is a significant concern for our diabetic patients. This effect was not seen in the CREDENCE trial, but more studies are needed to evaluate fully the extent of this risk. For now, Dr. Pham doesn’t prescribe these meds to patients with current diabetic foot ulcers. Some sources recommend caution in patients with known peripheral vascular disease as well.
Other potential risks include bone fractures, hyperkalemia, euglycemic DKA, Fournier’s gangrene, and UTIs.
The American Diabetes Association abridged their recommends considering these medications early in your patients with HFrEF (EF <45%) and CKD with GFR 30-60. They recommend consideration of these medications after starting metformin and lifestyle modifications regardless of baseline A1c or A1c target.
On Wednesday, we went over an interesting case of esophageal rupture with Dr. Vibha Mohindra. She took us through the case step by step, letting us hear her differential and how different pieces of data changed how she viewed the case and prompted her to ask different questions.
Our patient was an elderly gentleman with a history of diabetes, hypertension, and osteoarthritis on chronic NSAIDs who presented with days of progressive, nonspecific chest pain. Shortly after presentation, he had an episode of hematemesis and subsequently experienced rapid respiratory and hemodynamic decompensation, requiring emergency intubation, high doses of multiple vasopressors, and broad spectrum antibiotics. Subsequent imaging revealed a large left pleural effusion, which was found to be a Candida empyema after chest tube placement. Fungal empyemas are most commonly a postoperative complication of cardiothoracic surgery, but also occur in esophageal rupture. Interestingly, this patient’s pleural cytology later showed thick proteinaceous material intermixed with inflammatory cells and vegetable material. Gastrograffin swallow study revealed extravasation of constrast outside of the GI tract into the left pleural space and mediastinum, confirming a distal esophageal perforation. Cardiothoracic surgery was consulted for repair.
Esophageal perforation is an extremely rare, but potentially fatal diagnosis. 15% of esophageal perforations are considered spontaneous (Boerhaave’s syndrome). The following is our illness script for Esophageal rupture:
Epidemiology:
Signs/symptoms:
Diagnosis:
Treatment:
