
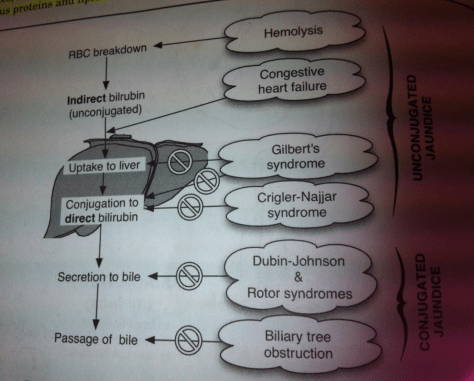
Remember to differentiate between causes of direct (conjugated) and indirect (unconjugated) hyperbilirubinemia:
Direct:
Gallstones
Intrinsic/Extrinsic Tumors (cholangiocarcinoma, pancreatic, HCC, etc.)
PSC / PBC
AIDS cholangiopathy
Strictures following invasive procedures
Parasitic infections: liver flukes
Viral hepatitis
Alcoholic hepatitis
Drugs/Toxins
Sepsis/Hypoperfusion
Infiltrative process (sarcoidosis, TB, lymphoma, amyloidosis)
Rotor syndrome
Dubin-Johnson syndrome
Indirect:
Extravascular/Intravascular hemolysis
Heart failure
Gilbert’s syndrome
Crigler-Najjar Syndrome
Hyperthyoidism
LFT abnormalities:
Cholestatic pattern: elevated bilirubin, high alk phos in relation to AST/ALT pattern
Hepatocellular pattern: elevation of AST/ALT in relation to alk phos and bilirubin levels.
Courvoisier’s Sign: palpable, non-tender gallbladder in a jaundice patient; cause is unlikely to be gallstone.
Cholangiocarcinoma:
Epidemiology: 8/million individuals, peak 50-70 years old; 2/3 Klatskin tumor (at bifurcation of left/right hepatic ducts), 1/3 intrahepatic
Risk Factors: PSC (1.5% per year), liver flukes
Clinical presentation: Ductal obstruction – jaundice (90%), pruritis (66%)
Ab pain (30-50%), weight loss (30-50%), fever (20%)
Treatment: Surgery – complete resection 40-60% 3 year survival; 10% operative mortality
Palliative – <18 month predicted mortality
