Inflammatory Neuropathies
Common Features:
1) Acquired, not inherited
2) Due to immune damage to peripheral nerves
Acute Disorders:
Acute Inflammatory Demyelenating Polyneuropathy (AIDP): incidence 1-2/100,000; 75-80% of acute fall into this category; symmetrical weakness/sensory loss over 1-4 weeks
Acute Motor Axonal Neuropathy (AMAN): AKA Chinese Paralytic Sydrome – similar to AIDP in onset, but without sensory changes
Acute Motor/Sensory Axonal Neuropathy (AMSAN): fulminate/severe form of GBS that develops over DAYS; results in paralysis and sensory loss due to severe axonal damage. More common in Central/South America due to trigger by Camtylobacter jejuni.
Miller Fisher Syndrome (variant of GBS) – 3 Features
1) Double vision from weak eye muscles
2) Wobbly/Ataxic walk or gait
3) Loss of DTRs
Chronic Disorders:
Chronic Inflammatory Demyelenating Polyneuropathy (CIDP): most common chronic inflammatory neuropathy, neurologic cousin to GBS; prevalence 8/100,000. Develops slowly over 2 months or longer with symmetric weakness or sensory changes. DTRs are lost in involved extremities. Monophasic illness over 1-3 years with relapsing/remitting course. Responsive to therapy (as oppose to GBS).
Multifocal Motor Neuropahty (MMN): RARE; asymmetric inflammatory neuropathy; slow/stepwise development of distal UE muscle weakness; sensory nerve fibers are not affected
Multifocal Acquired Demyelinating Sensory and Motor Neuropathy (MADSAM) AKA Lewis Sumner Syndrome: RARE variant of CIDP, similar to MMN with sensory changes; asymmetric weakness with sensory changes.
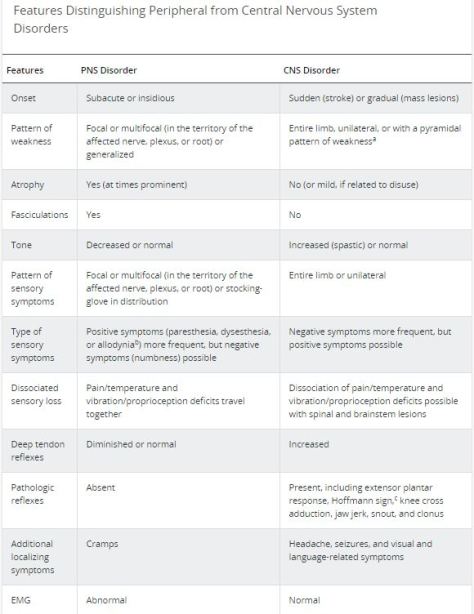
PNS versus CNS: