
Remember the different types of HIT:
|
|
Type 1 | Type 2 |
| Mechanism | Direct effect of heparin (non-immune) | Immune (Ab)-mediated IgG against platlet factor 4-heparin complex |
| Incidence | 10-20% | 1-3% with UFH; 0-0.8% with LMWH
|
| Onset | After 1-4 day of heparin therapy
|
After 4-10 day; but can occur <24 h if prior exposure w/in 100 days (persistent Ab). Postop highest risk. Can occur after heparin d/c’d
|
| Platelet nadir | >100,000/μL
|
~60,000/μL, ê 50%
|
| Sequelae | None | Thrombotic events (HITT) in 30-50%; rare hemorrhagic complications
|
| Management | Observe | Cessation of heparin, alternative non-heparin anticoagulation to prevent thrombosis
|
Pathophysiology:

- Autoantibodies (IgG) are formed to platelet factor 4 (PF4) complexed with heparin
- Platelet Fc receptors bind the antibody-heparin-PF4 immune complex
- Thrombocytopenia occurs by two mechanisms:
1) Platelet removal by splenic macrophages
2) Platelet consumption due to thrombus formation
Clinical Variability:
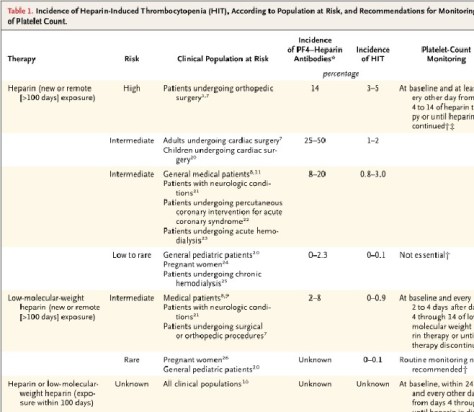
- 10 times higher incidence with UFH compared with LMWH
- A metaanalysis of 15 studies (>7000 patients) that evaluated the risk of HIT with prophylactic UFH vs LWM found the following absolute risks of developing HIT
- UFH – 2.6% (95% CI 1.5 – 3.8%)
- LMH – 0.2 % (95% CI 0.1 – 0.4%)
- Surgical > Medical patients; Incidence is particularly high after orthopedic surgery
Risk Factors:
- There is no dose of heparin that is too low to cause HIT! Patients have developed HIT after exposure to as little as 250 U flush.
- Female sex appears to be at a higher risk for unclear reasons – this was based on 7 trials comparing UFH vs LWH found approximately twice the risk.
Clinical Manifestations:
- Thrombocytopenia (<150,000/microL ~ 85-90%)
- Platelet drop of >50% is typical with mean nadir of 60,000/microL and RARELY <20,000/microL
- Typical onset is 4-10 days after heparin therapy
- Patients with exposure to heparin in the previous 100 days can develop a early onset (<24 hours) HIT
- Thrombosis occurs in up to 50% of HIT patients (venous > arterial); presenting finding in up to 25%
- Thrombotic sequelae – skin necrosis, limb gangrene, organ ischemia/infarction
4T Score:
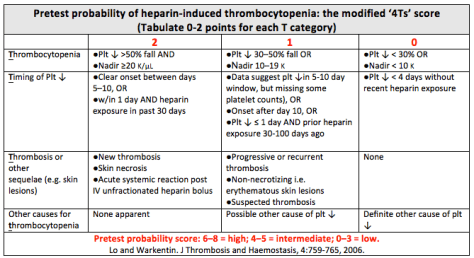
- A total score <4 points has a very high negative predictive value (97-99%); additional testing is not necessary
Assuming an intermediate/high risk score – what other labs can aid in the diagnosis:
- Anti-PF4 heparin antibodies – excellent NPV (98-99%), but low PPV due to presence of clinically insignificant antibodies (IgM, IgA)
- Our lab restricts the antibodies to only IgG – which increases the specificity
- Also provides an optical density (magnitude of anti-PF4-heparin reactivity) ~ greater activity (>2.0) correlates to a greater likelihood of HIT
- Serotonin-release assay – functional assay that measures heparin-dependent platelet activation; a negative result rules out HIT
Treatment:
Step 1: Immediate cessation of heparin
Step 2: : Initiation of an alternative anticoagulant at a therapeutic dose.
- Vitamin K antagonists should NOT be given until HIT has resolved (i.e. platelets > 150,000 for >2 days) because they increase the risk of venous limb gangrene/limb loss by decreasing levels of protein C.
- Argatroban (direct thrombin inhibitor) is the only currently FDA approved medication in the US. Danaparoid (anti-factor Xa) is approved in Canada, EU, and Australia. Other options include: Lepirudin and Bivalrudin.
