
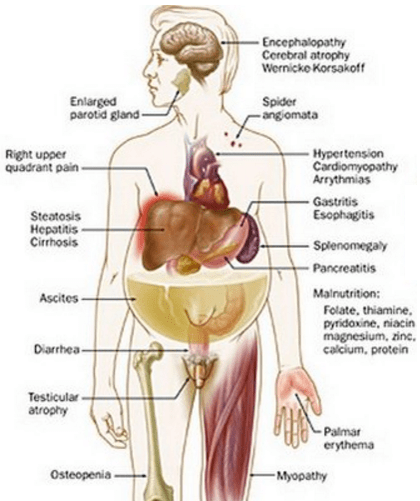
Some common physical exam findings of liver disease:
- Fetor hepaticus (breath smells like a freshly opened corpse)
- Spider nevi
- Gynecomastia
- Jaundice / Scleral icterus
- Ascites
- Caput medusae (dilated abdominal veins)
- Rectal varices
- Testicular atrophy
- Palmar erythema
- Dupuytren’s contracture
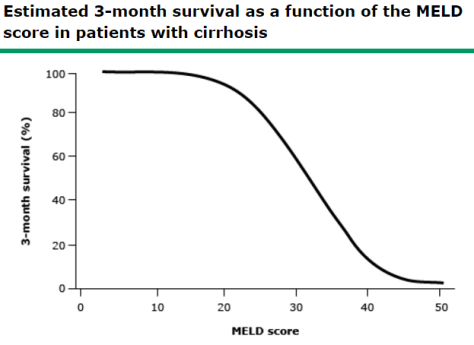
MELD Score:
- Predicts 3-month survival in patients with cirrhosis. In cirrhotic patients, an increasing MELD is associated with increasing severity of hepatic dysfunction and increased 3-month mortality.
Factors that go into MELD: serum bilirubin, serum creatinine, INR, sodium (added 1/2016), +/- hemodialysis > 2 in the past week
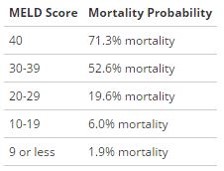
MELD Interpretation:
Maddrey Discriminant Function:
DF = (4.6 x [prothrombin time] – [control prothrombin time]) + (serum bilirubin)
- DF > 32 indicates SEVERE alcoholic hepatitis
- High short term mortality (20-30% within 1 month; 30-40% within 6 months)
- Patient may benefit from glucocorticoids
- Prednisone requires hepatic conversion to the active form (prednisolone)
- Multiple trials have showed a reduced short term mortality in patients with a DF >32 (NNT 3-68); no effect in patients <32
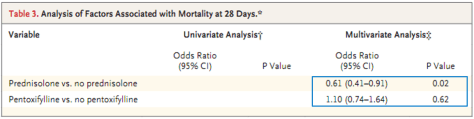
STOPAH Trial:
- Multicenter, double blinded, RTC
- 1103 patients with DF >32 and TBili > 4.7
- 4 treatment groups: (placebo, pentoxifylline + placebo, prednisolone + placebo, pentoxifylline + prednisolone)
- Prednisolone had a significant 28 day mortality benefit (after adjusting factors), but the benefit was lost at 90 days and 1 year
- Pentoxifylline did not improve survival compared to placebo
Hepatorenal Syndrome:
Characteristics of HRS:
- Clinically evidence acute or chronic liver disease
- Progressive rise in serum creatinine
- Normal urine sediment
- Absent/Minimal proteinuria
- Low urine sodium (often < 10 mEq/L)
- Oliguria
Types of HRS:
Type 1: more serious; at least a 2 fold increase in serum creatinine to >2.5 mg/dL in less than 2 weeks
Type 2: less severe; major clinical feature is ascites resistant to diuretics
Etiology:
- Splanchnic vasodilation ⇒ reduced effective circulating volume ⇒ renal failure
- MAP = CO x SVR; In patients with HRS, SVR is decreased (from splanchnic vasodilation); hence treatment is aimed at improving SVR and MAP.
Diagnosis of HRS is one of exclusion:
- Normal urinary sediment
- Absence of nephrotoxic meds
- No hypotension
- Urine studies similar to pre-renal AKI
Fluid challenge with albumin: 1 g/kg albumin (max 100 g) daily for 2 days
- If renal function IMPROVES, suggestive of pre-renal AKI
- If renal function continues to DECLINES, suggestive of HRS
Treatment of HRS:
- Liver transplantation – TREATMENT OF CHOICE
- Medical Management:
- ICU: treat with norepinephrine and albumin
- Non-ICU: treat with midodrine, octreotide, and albumin
