
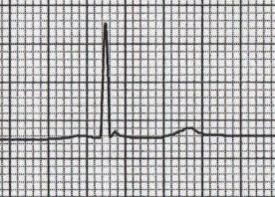
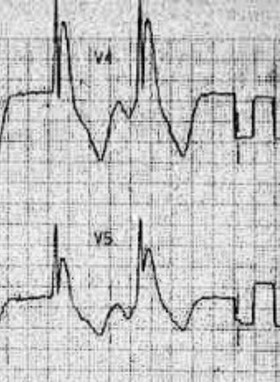
Osborn Waves (J Waves):
- The Osborn wave (J wave) is a positive deflection at the J point
- It is usually most prominent in the precordial leads
- Typically associated with hypothermia (typically < 30 C), but they are not pathognomonic; Also seen in: hypercalcemia, neurological insults, medication side effect
- Height of the Osborn wave is roughly proportional to the degree of hypothermia
32.5 C
30 C

<27 C
Thyroid Regulation:
- TRH (a tripeptide amide) formed in the hypothalamus and travels to the anterior pituitary where it stimulates the release of TSH.
TSH has 3 main effects:
- ↑ release of preformed thyroid hormone
- ↑ formation of thyroid hormone
- ↑ size/number of thyroid cells
Synthesis of T3 and T4 (very complicated) requires two main components thyroglobulin and iodine.
4 physiologic effects of T3 and T4:
- ↑ basal metabolic rate (↑ heat generation, ↑ O2 consumption)
- ↑ metabolism (↑ gluconeogenesis, ↑ glycolysis, ↑ glucose absorption, ↑ lipolysis, ↑ protein turnover)
- Stimulates bone maturation and growth
- ↑ cardiac output (↑ HR, ↑ contractility)
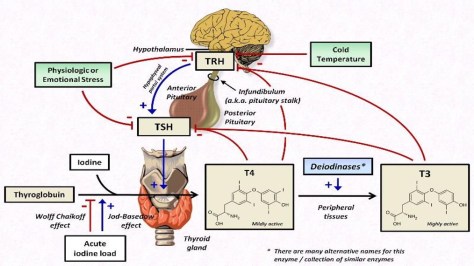
Wolff Chaikoff effect: reduced thyroid hormone following large ingestion of iodine; explains potential hypothyroidism cased by amiodarone.
Jod-Basedow effect: iodine-induced hyperthyroidism in a patient with an endemic goiter
Myxedema Coma:
3 key features:
- Altered mental status: despite the name, most patients do not present in coma, but usually with confusion/lethargy
- Hypothermia: due to decrease in thermogenesis that accompanies the decrease in metabolism
- Precipitating event: look for cold exposure, infection, drugs (diuretics, sedatives, analgesics), trauma, stroke, heart failure, GI bleed, etc.
Pathogenesis:

Typical presenting patient: older female presenting in the wintertime (often with a history of hypothyroidism)
- Female > Male 4:1
- Almost exclusively > 60 years old
- 90% of cases during the winter months
If diagnosis is suspect, labs to get include:
- TSH
- FT4
- Cortisol
Pearl: without a frankly low T4 level, myxedema coma is unlikely, regardless of the TSH elevation
Myxedema coma is an endocrine emergency and should be treated aggressively – mortality rate 20-40%
Treatment:
- Thyroid replacement – controversial about type of replacement: Levothyroxine (T4) versus Liothyronine (T3), but initially route of administration should be IV given potential for impaired GI absorption
- Stress dose steroids – patients with secondary hypothyroidism may have associated hypopituitarism and secondary adrenal insufficiency
- Supportive measures – ICU management, mechanical ventilation (if necessary), IVF, vasopressors, rewarming, etc.
