
Pneumocystis jiroveci pneumonia (PJP):
– opportunistic infections are the most common etiologies of infection in patients 1-6 months after solid organ transplant.
Common signs/symptoms of PJP:
– Progressive exertional dyspnea (95%)
– Fever (90%)
– Non-productive cough (90%)
Pearl: walk patients with suspected PCP to reveal hypoxemia!
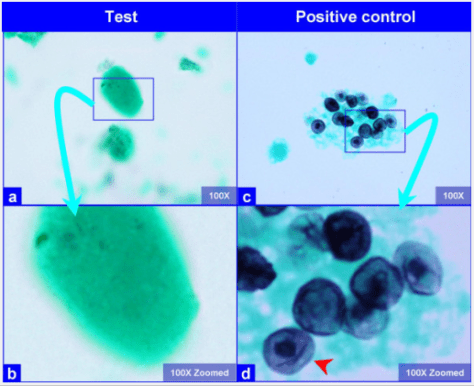
Diagnosis:
– Direct fluorescent antibody stain (DFA stain)
– Gomori methenamine silver stain (GMS stain)
*Must visualize the cystic/trophic forms directly
Treatment: TMP/SMX for 21 days
– Add steroids for pO2 ≤ 70 or A-a gradient ≥ 35
Toxic Shock Syndrome:
– expect a TSS board question to present as overwhelming sepsis in the context of a menstruating female or a post-surgical wound infection
– toxins (called super antigens) stimulate cytokine production, resulting in systemic signs of shock
Triad of TSS:
– Shock
– Fever
– Rash – diffuse macular rash with subsequent desquamation, especially on the palms and soles
*Along with involvement of at least 3 organ systems

Organisms often involved:
– S. aureus
– S. pyogenes
Treatment:
S. pyogenes: penicillin plus clindamycin
MSSA: Nafcillin or oxcillin plus clindamycin
MRSA: Vancomycin plus clindamycin
* add clindamycin to suppress protein synthesis and, therefore, toxin production
Scarlet Fever:
Key features:
– “circumoral pallor” – pale area around mouth
– “Pastia lines” – petechial lines in the skin creases
– desquemation
Most common organism: Group A Streptococcus
5 “S'” of Scarlet Fever:
– Streptococci (causative organism)
– Sorethorat
– Swollen tonsils
– Strawberry tongue
– Sandpaper rash
Treatment: Oral penicillin V; amoxicillin, 1st generation cephalosporins, and IM PCN G are alternatives
Lyme Disease:
– Erythema migrans is the associated rash

– Borelia burgdorferi is the causitive organism and Ixodes tick is the vector
– > 95% of cases occur in regions where the Ixodes tick is abundant

Other infections spread by Ixodes tick:
– Babesiosis
– Anaplasmosis
Signs/Symptoms of different stages of Lyme disease:
Localized: erythema migrans (target lesion at site of tick attachment ~ 60-80%), fever/other systemic symptoms are rarely present
Early disseminated: erythema migrans at multiple sites, febrile illness with constitutional symptoms (myalgia, arthralgia, and headache)
Cardiac: asymptomatic PR prolongation → complete heart block
Neurologic: facial nerve palsy (most common) either unilateral or bilateral
Late disseminated: oligoarticular inflammatory arthritis involving large joints (i.e. knee)
Rocky Mountain Spotted Fever:
Look for a history of exposure to ticks in endemic areas (southeast / south central US) and features of:
– Pancytopenia (esp thrombocytopenia)
– Hyponatremia
– No evidence of DIC (normal PT/PTT)
– ↑ transaminases

Rash of RMSF:
– >85% of patients by 1 week
– May lag behind other symptoms (~50% by day 3)
– Typically starts at the distal extremities and progress centrally; involves the palms/soles in >30% and typicially spares the face
Treatment:
– Doxycycline; choloramphenicol is an alternative option in pregnancy
Ehrlichiosis:
Think of Ehrlichia as “Rocky Moutain spotless fever”
– presents similarly to Anaplasmosis
– endemic to the southcentral and southeastern US
– spread via the Lone Star tick
Symptoms in order of frequency:
Fever (~90%) > headache > myalgia > arthralgia > meningismus
– Blood smear can help with visualization of intracytoplasmic inclusions in WBCs; only present in ~30%
Treatment:
– Doxycycline
Coccidioides Infection (Valley Fever):
– Clues to be aware of: Arizona/New Mexico and erythema nodosum
– Endemic to SW US (Arizona, New Mexico, Texas, and central valley of California)
– Route of infection: inhalation of fungal particles found in the sand
– Arthralgia of multiple joints “desert rheumatism” is common.

Diagnosis confirmed on fungal stains
– Thick walled spherules (10-80 uM) with endospores are seen in tissue

No treatment for mild disease; use itraconazole or fluconazole for severe illness
Histoplasmosis:
Exposure history is key here; think of histo with any of the following exposures in the SE/SC US:
– Bats (or guano)
– “Spelunking” (cave exposure)
– Farm buildings / bird-roosting locations

Most infections are subclinical (~95%); can see mucocutaneous lesions
Antigen detection in urine great for disseminated infections (>85%)
Blastomycosis:
– Endemic to Ohio and Mississippi/ River valleys
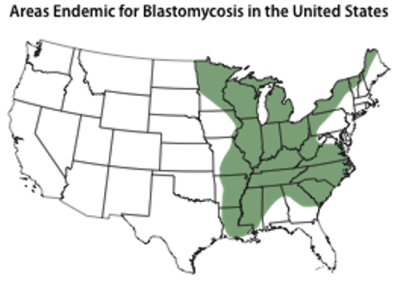
– Primarily a pulmonary infection, may disseminate to the skin and bone
– Well demarcated skin lesion is most common manifestation of disseminated disease

– Appears as a broad based budding pattern at 37 C


Hi, the Erythema migrans rash of Lyme disease is not just a “target”. The central clearing is an ATYPICAL manifestation. Only 20% of Lyme rashes have central clearing, which means only 1 in 6 patients has a bulls eye rash. Only 70-80% at most of Lyme disease patients have any rash at all.
LikeLike