
| Infection | CD4 Count | Prophylaxis |
| PCP pneumonia | < 200 | TMP-SMX |
| Toxoplasmosis | < 100 | TMP-SMX |
| MAC | < 50 | Azithromycin |
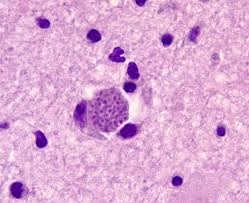
Toxoplasmosis:
Presumptive Diagnosis: *usually made to avoid brain biopsy
- CD4 < 100
- Lack of effective prophylaxis
- Clinical syndrome (headache, neuro symptoms, fever, etc.)
- + T. gondii IgG antibody
- Imaging consistent with disease (multiple ring-enhancing lesions)
* If present >90% probably of TE.
Definitive Diagnosis:
- Clinical syndrome (headache, neuro symptoms, fever, etc.)
- Identification of ≥ 1 mass lesion by brain imaging
- Detection of organism in biopsy specimen
Treatment:
- Sulfadiazine
- Pyrimethamine
- Leucovorin – to prevent pyrimethamine induced hematologic toxicity
- Measure response to treatment with daily neurological exams and repeat neuroimaging after 2-3 weeks
- 75-80% of patients with TE will show radiographic and/or neurologic improvement
- Treat for 6 weeks followed by maintenance therapy
ART:
- 3 drugs from 2 different classes
- Usually 2 nucleoside RTIs “backbone” and 3rd agent – either a protease inhibitor or an integrase inhibitor
Post-Exposure Prophylaxis:
- Started immediately after exposure => continued for 4 weeks
- Test immediately, 6 weeks, 12 weeks, and 6 months
- 3 Drug Regimen: Tenofovir-Emtricitabine + Raltegravir
Pre-Exposure Prophylaxis:
- Recommended for certain high-risk populations: heterosexual partners of infected patients, MSM, IVDU
- 2 Drug Regimen: Tenofovir-Emtricitabine
