
Clinical presentation of SAH
–THUNDERCLAP headache (!)- 97 % present with sudden onset severe HA-worse headache of their life.
-Can be associated with LOC (if severe), nausea, vomiting, meningismus, CN deficits, seizures (10 %), and SUDDEN DEATH (10-15 %)
-30-50 % have a sentinel headache preceding SAH
Making the diagnosis
-Always start with non-contrast HEAD CT
-Picks up 92 % of SAH if <24 hours but sensitivity is highest in first 6-12 hours after SAH (~nearly 100 %!) but drops to about 60 % by 5d.
-If negative, proceed with LP ~12 hours later (may be falsely negative early)
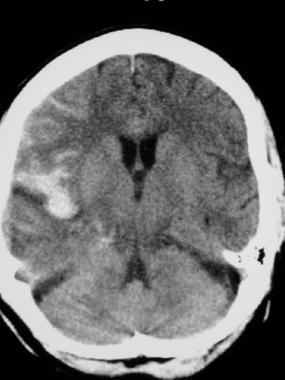
- SAH on CT scan
What do you see on LP if SAH?
-Elevated opening pressure
-Significantly elevated RBC count with bloody tap that does not clear (although RBC count can go down) so not always helpful to distinguish from traumatic tap
–Xanthochromia (pinkish-yellowish tint)-due to hemoglobin degradation products and means blood has been in the CSF for at least 2 hours
Excellent sensitivity/specificity if done <12 hours from SAH but can also see Xanthochromia if high protein content, systemic bilirubin>15, and very traumatic tap (RBC>100k)

Etiologies of non-traumatic SAH (not a complete list)
–ANEURYSMS (Most Common)
–Perimesencephalic
-Vascular malformations
-Arterial dissection
-Cerebral venous thromboses
-Cocaine abuse
-In setting of anticoagulation
-Reversible Cerebral Vasoconstriction Syndrome (RCVS)
Complications of SAH
51 % die from SAH so very high mortality
–Rebleeding (highest in first 24 hours)
–Hydrocephalus (early)-May need VP shunt
-Vasospasm (delayed cerebral ischemia)
-Increased ICP
–Seizures-May need AEDs
–Cardiac Arrhythmias
Treatment
-If aneurysm-treat with surgical clipping or endovascular coiling.
-Prevent vasospasm with Nimodipine 60 mg PO q4h
