
Classic Triad of Infectious Mono
-Fever
-Pharyngitis
-Lymphadenopathy
*Most common symptoms however are MALAISE and SORE THROAT. Less common but if you see Palatal Petechiae, think about Mono!
Epidemiology
-Most common in adolescents aged 10-19 but can be seen in adults as well
Etiology
-EBV (Epstein Barr Virus)-90-95 % people are EBV seropositive but long latency period.
-Spread by Saliva and sexual transmission (not just the kissing disease)
Diagnosis
-Heterophile antibodies (Monospot is using Horse RBC agglutination)
Sensitivity=85 % while Specificity=97-100 % (can be falsely negative up to 25 % in first week so VCA may be more helpful)
-VCA (Viral Capsid Antigen) IgG, IgM
-Peripheral smear may show >50 % lymphocytes with atypical lymphocytes (see below)

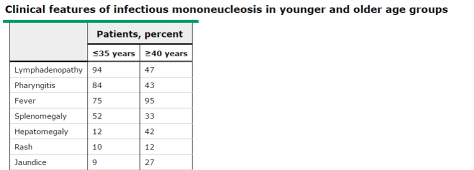
Signs and Symptoms
–Presentation differs depends on whether young or old as those in older groups have more atypical presentations (see below) including neutropenia and severe infection like our patient had!
Differential Diagnosis
Always keep Acute HIV infection in mind if you are thinking Mono but also includes Strep pharyngitis, Acute CMV, Toxoplasmosis, and Viral Pharyngitis.
Treatment
-Supportive care, hydration, NSAIDs/APAP use PRN
-No benefit to support routine use of H2 blockers, Acyclovir, or steroids although Acyclovir can decrease shedding time of virus
-4 weeks no contact sports (due to very low risk of splenic rupture) but they do NOT need to be on bed rest.
-Avoid ampicillin/amoxicillin as can classically cause a morbilliform rash
Further reading
