
Syncope
-Defined as ABRUPT and TRANSIENT loss of conscious associated with loss of postural tone followed by complete and RAPID spontaneous recovery
-Before you start working up syncope, make sure it is not a mimic like a seizure!
How do you make the diagnosis?
-Keep in mind that the majority of syncopal episodes are of unknown etiology but the most common known etiology is neurocardiogenic or vasovagal syncope. Despite what you saw on that episode of Scrubs, this type of syncope is not diagnosed with a blood test
-A detailed H&P makes the diagnosis in about 50 % of patients with syncope, especially focusing on whether it was EXERTIONAL, Prodromal symptoms, changes in position during event, FAMILY HISTORY of sudden cardiac death, and any associated cardiac symptoms.
–Check orthostatics and EKG on everyone (still low yield but minimal cost and EKG can help you look for more dangerous etiologies)
–Telemetry is reasonable and recommended if you suspect a cardiac etiology for the syncope based on the H&P and EKG
-Do NOT get brain imaging (CT/MRI) in simple syncope as the yield is extremely low unless high suspicion for intracranial mass
-Echocardiogram and carotid ultrasound are also extremely low yield unless EKG or exam shows concerning features (eg: ejection murmur on exam concerning for AS, young male with severe LVH concerning for HOCM, bilateral carotid bruits)
-See below for common causes of syncope, diagnostic testing, and treatment (from Medscape)
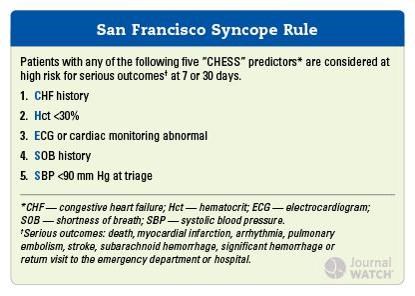
What is the San Francisco Syncope Rule?
-One of the many prognostic rules to look at whether someone is at high risk for serious outcomes and may need to be admitted if they meet ANY of these criteria
-If they meet NONE of the criteria with no other obvious source of syncope (eg: melena on exam), high NPV for serious outcomes from syncope at 7 or 30 days.
Conditions to look out for on an EKG of a young patient with Syncope
-HOCM
–Long QT syndrome (acquired or congenital) as increased risk of Torsades
-Brugada Syndrome
-Arrhythmogenic right ventricular dysplasia (ARVD)
-Arrhythmias
-Tachyarrhythmias (esp. VT but also WPW)
-Bradyarrhythmias (eg: heart block)
Workup of suspected LQTS
-Rule out secondary etiologies of prolonged Qtc (long list but includes many electrolyte abnormalities as well as DRUGS). BRADYCARDIA prolongs the QT interval.
-LQT1-LQT13 genetic testing as determining genotype can affect clinical course
-GXT testing to look for arrhythmias as well as monitor QT interval (normally decreases with increased HR but not always in LQTS)
Treatment
–Beta Blockers FIRST LINE but at higher risk for heart block
-Keep Mg and K at normal limits to avoid Qtc prolongation, avoid drugs that can worsen prolongation
-PPM, left cardiac sympathectomy, and AICD may be needed
-Referral to center with radiofrequency catheter ablation.
