
Thanks to Joe for presenting the case of a young man with no known medical history who presented with acute onset of generalized weakness, found to have symptomatic hyponatremia to 120 resulting from psychogenic polydipsia!
Clinical Pearls
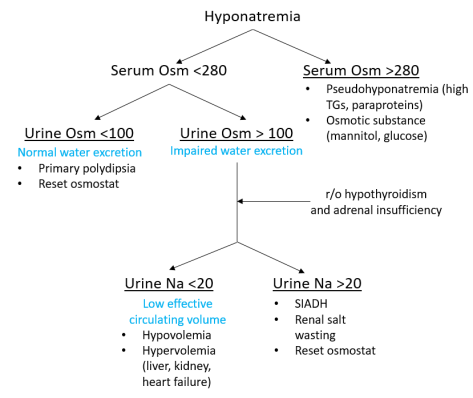
- Hyponatremia is largely a problem of too much free water (sometimes compounded by too little solute) and defined as a Na <135
- Pick a systematic approach to solving the underlying diagnosis for any patient with hyponatremia (see below for one possible outline).
- The term “pseudohyponatremia” refers to the presence of substances that interfere with laboratory measurement of sodium concentration in the blood, specifically high triglycerides and paraproteins.
- Hyperglycemia does NOT fall into this category because glucose is osmotically active and pulls water into the intravascular space, resulting in a dilutional and true hyponatremia.
- Chronic hyponatremia (>72 hours) must be corrected slowly to avoid osmotic demyelinating syndrome (ODS). Acute hyponatremia (<48 hours) can be corrected more rapidly. That said, we rarely have a Na value within 48 hours prior to patient presentation to determine acuity. As a result, and given the neurologic risks, most patients are treated as if they have chronic hyponatremia.
- ADH leads to increased uric acid excretion through the kidneys so low serum uric acid levels have been associated with SIADH. But this test is not very specific.
- Osmolarity of normal saline is 308 compared to human serum which is normally 280-295. In a hyponatremic patient, NS infusion becomes a relatively hypertonic (rather than isotonic) solution!
For more detailed information, refer to this prior post and this review article.

One thought on “Hyponatremia – 9/18/18”