
Yours truly presented a case of a middle-aged woman with a recent history of otitis, sore throat, conjunctivitis, photophobia, and arthralgias who presented with chronic and progressive decline in functional status and AMS, found to be uremic with work up revealing c-ANCA associated ESRD.
Clinical Pearls
- Remember that oval fat bodies are specific for glomerular pathology (more commonly nephrotic syndrome but can be seen in nephritic disease as well).
- ANCA-associated vasculitides include GPA, MPA, eGPA (and renal-limited vasculitis).
- All have similar features on renal histology (focal necrotizing, crescentic, pauci-immune glomerulonephritis).
- They can affect multiple organ systems (see breakdown below) which makes their clinical diagnosis challenging apart from the following differences:
- c-ANCA is associated with GPA, p-ANCA is seen in MPA and eGPA
- Granulomas are seen in GPA and eGPA
- Eosinophilia and asthma are associated with eGPA
ANCA-associated vasculitides
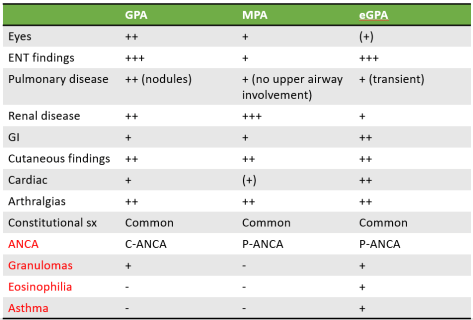
Chart above adapted from this paper by Koldingsnes et al.
Granulomatosis with polyangiitis (GPA)
Diagnostic criteria (two or more has 88% sensitivity and 92% specificity):
- Nasal or oral inflammation (painful/painless oral ulcers, or purulent or bloody nasal discharge)
- Abnormal chest radiograph showing nodules, fixed infiltrates, or cavities
- Abnormal urinary sediment (microscopic hematuria w/w/o red cell casts)
- Granulomatous inflammation on bx of artery or perivascular area
Clinical presentation:
- Most commonly in older adults, M=F
- More common among white individuals (~89%)
- S/s
- Fatigue, fever, weight loss, arthralgias, rhinosinusitis, cough, dyspnea, urinary abnormalities, purpura, and neurologic dysfunction.
- ENT
- 90% of GPA cases, only 35% of MPA
- Nasal crusting, sinusitis, otitis media, earache, polychondritis, ulcers, discharge
- Conductive and/or sensorineural hearing loss
- Saddle nose deformity
- Tracheal and pulmonary disease
- Airways or parenchyma
- Renal
- ~18% at presentation but subsequently develops in 77-85% of patients within the first 2 years of disease onset
- High risk of progression to ESRD
- Asymptomatic hematuria
- Subnephrotic range proteinuria
- Rapidly progressive GN
- Cutaneous
- ~50% of patients
- Leukocytoclastic angiitis is most common which causes purpura of lower extremities
- Other findings: urticarial, livedo reticularis, nodules, erythema nodosum, pyoderma gangrenosum, and Sweet syndrome
- Ophthalmic/orbital
- Conjunctivitis, corneal ulcers, episcleritis/scleritis, optic neuropathy, retinal vasculitis, and uveitis.
- Other organs
- CNS: neuropathy, CN abnormalities, mass lesions, hearing loss, granulomatous inflammation of the CNS
- GI tract, heart, lower GU, parotids, thyroid, liver, or breast
- High incidence of DVT (unclear mechanism)
- Can progress slowly over months or explosively over days
- Relapses can manifest differently than original presentation
Diagnosis requires biopsy!
Treatment:
- Prompt initiation of therapy can be life and organ sparing
- Induction therapy: Steroids +-Cyclophosphamide +-Rituximab
- Maintenance therapy: multiple options-Azathioprine, MTX, Rituximab, Leflunomide
