
Shout out to Paige for admitting the interesting young woman with no medical history who presented with blurry vision, found to be in hypertensive emergency and nephrotic syndrome. Her work up revealed diffuse proliferative lupus nephritis (class IV) without any other clinical features of lupus!
Clinical Pearls
- Proteinuria is primarily caused by three processes: 1) overflow (due to elevated paraprotein levels), 2) glomerular disease, 3) tubular disease (rarely reaches nephrotic range)
- Renal involvement is noted in ~50% of patients with SLE and can present as nephrotic and/or nephritic syndromes.
- The most common and severe form is diffuse proliferative lupus nephritis (class IV)
- Keep in mind that SLE flare is associated with a normal/low WBC, normal/low CRP, and absence of fever. Infection, which can instigate a lupus nephritis flare, would cause an elevated WBC, elevated CRP, and fever.
- Lab findings suggestive of SLE flare also include an elevated anti-dsDNA (correlates with disease activity), low complement levels (especially C3), worsening proteinuria, and elevated creatinine.
- Treatment involves an induction phase with cytoxan or MMF plus solumedrol followed by a maintenance phase with the goal of reducing urine protein excretion to <0.33 g/day.
Hypertension urgency/emergency:
- Urgency: BP>180/120 without end organ damage
- Manage with orals, goal to lower (not necessarily correct) over 24-48 hours
- Emergency: elevated BP + end organ damage (brain, eye, heart, kidney)
- Manage with IV meds, reduce DBP by 10-15% over the first hour, then by 25% over the next 6-12 hours.
- Special situations:
- Lower rapidly in acute aortic dissection (goal SBP <110 ASAP)
- Recent ischemic stroke: do not lower BP unless > 220/120 (> 185/110 if received reperfusion therapy)
Lupus
- Female to male prevalence is 9:1
- Diagnose using Systemic Lupus International Collaborating Clinics (SLICC) criteria. Must have > 4 (at least 1 clinical and 1 laboratory) OR biopsy proven lupus nephritis with a positive ANA or dsDNA
- Autoantibodies:
- dsDNA is 50% sensitive but 97% specific –> can monitor disease activity
- Smith is 10-20% sensitive but >90% specific
- Work up of presumed flare:
- Important to distinguish flare from acute infection but keep in mind that infection can trigger flare
- SLE flare:
- Low WBC and normal CRP (except when serositis is present)
- Fever is unusual
- Infection:
- High WBC and high CRP
- Fever is common
- Treatment:
- Plaquenil for all unless contraindicated
- Mild/mod:
- plaquenil, NSAIDs, low dose steroids (pred 5 daily)
- Severe
- Acute: high dose steroids
- Chronic: Immunosuppressive agents (MTX, cyclosporine, cyclophosphamide, azathioprine, mycophenolate, belimumab)
- Prognosis
- Worse with pediatric onset, ethnic minority, renal involvement, increased number of diagnostic criteria, low complement, e/o end organ damage
- High association of CVD and SLE
SLE and renal disease
- Renal involvement is common and eventually occurs in ~50% of SLE patients
- 10% progress to ESRD
- High mortality compared to SLE without nephritis
- More common and severe in African Americans, Hispanics, Asians
- Classifications of GN: can evolve from one to another
- Minimal mesangial lupus nephritis (class I)
- Earliest and mildest form
- Rarely diagnosed b/c pts have a normal U/A, no or minimal proteinuria, and normal Cr
- Mesangial proliferative lupus nephritis (class II)
- Microscopic hematuria and/or proteinuria
- Light microscopy would show mesangial hypercellularity or mesangial matrix expansion
- Focal lupus nephritis (class III)
- Hematuria, proteinuria, some HTN, decreased GFR
- Less than 50% glomeruli affected by light microscopy
- Segmental glomerulonephritis
- A: active lesions –> focal proliferative
- A/C: active and chronic lesions –> focal proliferative and sclerosing
- C: chronic inactive lesions and scarring –> sclerosing
- Diffuse lupus nephritis (class IV)
- Most common and most severe
- Hematuria, proteinuria, nephrotic syndrome, HTN, reduced GFR
- Hypocomplementemia (esp C3) and elevated anti-dsDNA during active disease
- >50% of glomeruli are affected
- Lupus membranous nephropathy (class V)
- nephrotic syndrome, Cr normal or slightly elevated
- Diffuse thickening of the glomerular capillary wall and subepithelial deposits
- Can present without any other clinical or serologic manifestations of SLE
- Advanced sclerosing lupus nephritis (class VI)
- Slow, progressive renal dysfunction with proteinuria and relatively bland urine sediment
- Global sclerosis >90% of glomeruli
- Active GN no longer observed
- Minimal mesangial lupus nephritis (class I)
- Treatment:
- Best to initiate early
- Aimed at proliferative lupus nephritis
- Induction
- 3 – 12 months: goal is to obtain renal response.
- Cytoxan or MMF PLUS solumedrol 250-1 g/day x 3 days (former takes 10-14 days to have an effect so the latter is much faster) or prednisone 60 mg/day
- Maintenance
- Response:
- substantial reduction in urine protein excretion to <0.33 g/day
- improvement or stabilization of serum creatinine
- improvement of urinary sediment
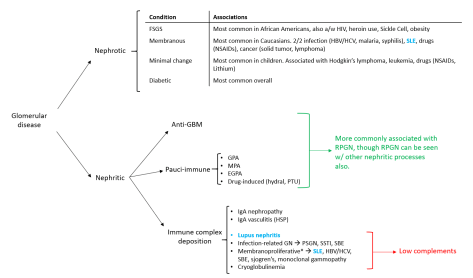
Approach to glomerular disease:

One thought on “Lupus Nephritis”