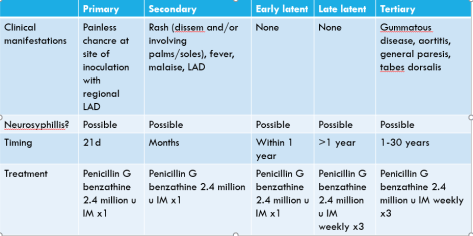
Today’s case, brought to us by Dr. Tuan Nguyen, was a middle-aged woman who presented with sore throat and globus sensation, which persisted for >6 weeks before she received a tonsilar biopsy that showed Treponema pallidum, consistent with secondary syphilis.
We went over a strategy of evaluation of the adult patient with acute pharyngitis. First, we ruled out any emergency by evaluating for airway compromise (respiratory distress, tripoding, “sniffing,” stridor), signs of epiglottitis or deep neck space infection (muffled/hot potato voice, drooling, bulging of the structures of the pharynx or palate, torticollis, neck pain/stiffness/swelling, trismus), or sepsis. We then evaluated for the likelihood of Group A strep infection with the Centor criteria. If left untreated, group A strep pharyngitis can lead to rheumatic fever, rheumatic heart disease, glomerulonephritis, and abscess. Then, we took a detailed sexual history to risk stratify the patient for acute HIV, gonococcal pharyngitis, and syphillis.