
Our wonderful medical student Tae presented a very interesting case today: a middle-aged male with no past medical history who presented with acute left knee pain and effusion, fevers, and leukocytosis.
With any monoarticular, painful joint effusion without a history of trauma, arthrocentesis should be performed to rule out septic arthritis and look for crystalline arthropathies (gout and pseudogout). This patient’s synovial fluid showed 10 thousand WBCs with >75% neutrophils.
Interpretation of synovial fluid studies: When interpreting synovial fluid studies, many factors should be taken into consideration. The general cutoffs for WBC count in the fluid are guidelines, but there is significant overlap between categories.
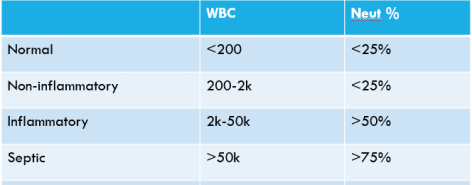
When differentiating between noninfectious inflammatory arthritides and septic arthritis, the distinction is not clear cut. The more WBCs you see in the joint fluid, the more likely it is to be a septic joint (>50,000 WBC is typical), but immunocompromise can decrease the WBC count and early in the course of septic arthritis, counts may be lower. Noninfectious inflammatory arthritis can have WBC counts >50,000 as well so history and other clinical data must be taken into account.
In this patient’s case, the WBC count of only 10 thousand falls in the classical non-infectious, inflammatory arthritis range. Gram stain did not show any organisms, but cultures grew rare growth Strep viridans and Actinomyces after more than 3 days in the micro lab. Outside of hematogenous spread of polymicrobial bacteremia and direct penetrating trauma to the joint, polymicrobial septic arthritis is exceedingly rare. Although all of this cast doubt on the diagnosis of septic arthritis, the patient was treated with Vancomycin and Zosyn initially, then narrowed to Zosyn alone. However, fevers continued, WBC count rose from 21 to 31, and procalcitonin increased from 0.83 to over 5. A second arthrocentesis was performed, which showed a WBC count of only 30 thousand and no organisms on gram stain with a negative culture. He was subsequently taken to the operating room for arthroscopic drainage and debridement, which did not yield any pus. The orthopedic surgery team deemed the knee to not be a septic joint and did not think bacterial joint infectious could be responsible for his worsening condition.
On review of systems, the patient also endorsed some mild left elbow pain and joint swelling over the past two weeks that had now resolved. A mild transaminitis was also observed on admission labs with extremely elevated CRP and ESR. During the admission, his right knee began to hurt and XR revealed another small effusion. He subsequently developed a diffuse, maculopapular rash, which was thought to be a drug rash. He was switched from Zosyn to Ceftriaxone and then again to Clindamycin, but the rash, fevers, and leukocytosis persisted. Tests for gonorrhea, chlamydia, HIV, syphilis, and viral hepatitis were all negative. Fungal and anaerobic cultures of synovial fluid were negative. Blood cultures did not show any growth and echocardiogram did not show any abnormalities or vegetation. ANA and anti-CCP were negative, and rheumatoid factor was only very weakly positive (only mildly above the upper limit of normal).
Finally, his ferritin came back at >17,000 and the diagnosis of Still’s disease was made. Still’s is a rare rheumatologic condition akin to juvenile rheumatoid arthritis. It is an out of control immune reaction that typically presents with daily or twice daily fevers, an evanescent salmon-colored maculopapular rash, and polyarticular arthritis. It can also cause severe nonsuppurative pharyngitis, liver dysfunction, pleural effusions, pericarditis, lymphadenopathy, and splenomegaly. The Yamaguchi criteria can be used to diagnose it after infectious, malignant, and other rheumatologic causes are ruled out. It is treated with high dose steroids and sometimes IL-1 or IL-6 inhibitors.
After this patient begun high dose steroids, his fevers and rash resolved, transaminitis slowly improved, and his arthritis became less severe, confirming the diagnosis of Still’s disease.
