We presented a very interested case of a healthy young female presenting with hemoptysis, hematuria, anemia and profound AKI concerning for RPGN + DAH (diffuse alveolar hemorrhage). Our patient had a stat kidney biopsy with serum studies that resulted in p-ANCA +, ANA +. Kidney biopsy resulted in light microscopy showing “Pauci Immune GN” or “Anti GBM GN” however conflicting IF results of “full house” immunostaining consistent with lupus nephritis. The patient was diagnosed with RPGN 2/2 likely p-ANCA vasculitis (MPA) WITH overlapping features of lupus nephritis. Patient improved w/ pulse dose steroids and Rituximab.
Advanced kidney disease on presentation should make you think of:
First think of pre-renal and post-renal etiologies but if intra-renal etiology of AKI is top of your differential, first start by considering the following:
- Pigment – Myoglobin (Rhabdo); Hemoglobin (aka Thrombotic Microangiopathy)
- Paraprotein – Multiple Myeloma (SPEP)
- Crystals – Tumor Lysis Syndrome (Uric Acid)
How to interpret UA
The UA is CRUCIAL in differentiating whether your AKI is glomerular, tubular, interstitial or vascular in etiology. When looking at UA, clues that this is a glomerular cause includes hematuria and proteinuria. Remember that the dipstick UA (3+) mainly measures albumin. Checking protein:creatinine urine helps you know if there are proteins besides albumin at play!
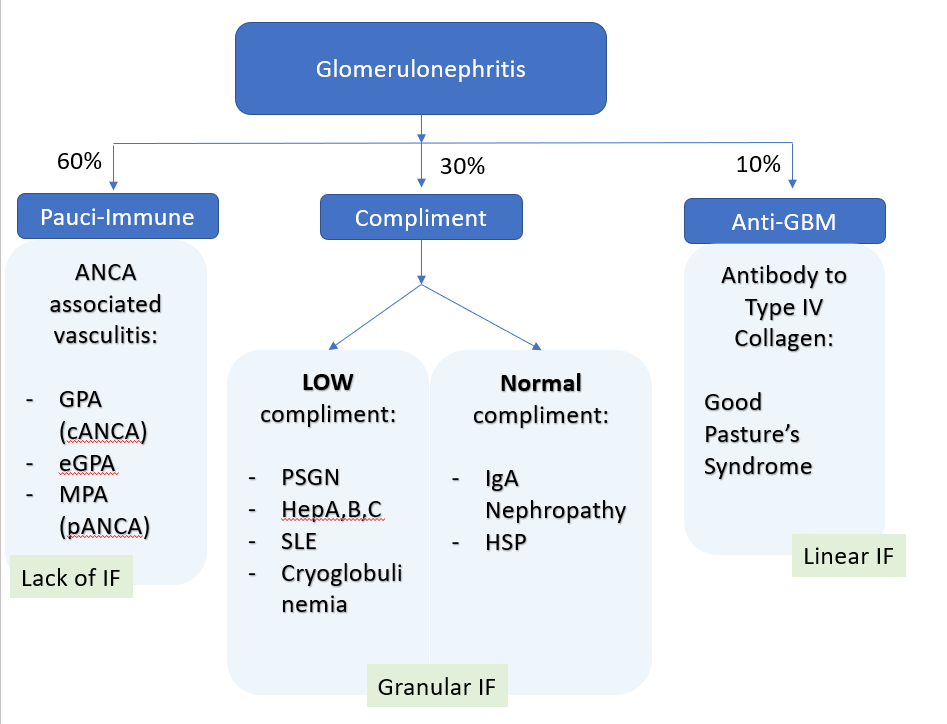
Glomerular causes of intrarenal AKI
The frank hematuria and amount of RBC clues us into a nephritis (rather than nephrotic) etiology as follows.