
We discussed a case of an elderly woman with history of HTN and pre-diabetes, who presented with acute hypertensive emergency and dizziness, found to have evolving EKGs (ST elevations in anterior/lateral precordial leads) and elevated troponins concerning for STEMI, due to Takotsubo cardiomyopathy.
Takotsubo cardiomyopathy
- Transient regional LV systolic dysfunction
- Absence of angiographic evidence of obstructive CAD or acute plaque rupture
- Affects women > men
- Typically seen in older adults (~60s)
Pathogenesis
- Pathogenesis is not completely known, but theorized to be due to catecholamine excess. This leads to diffuse catecholamine-induced microvascular spasm / dysfunction.
Signs and symptoms
- Physical or emotional stress trigger (not always present! one study reported lack of stress trigger in 28.5% of cases)
- Presents like ACS
Complications to watch out for
- Heart failure
- Arrhythmias
- Mitral regurgitation
- Cardiogenic shock, cardiac arrest
- Stroke (embolization from an apical thrombus that forms due to severe systolic heart failure)
Workup
- EKG findings
- ST elevations (most common) >>> ST depressions > other nonspecific findings (e.g. QT prolongation, T wave inversions)
- Elevated troponin
- Elevated NT pro-BNP
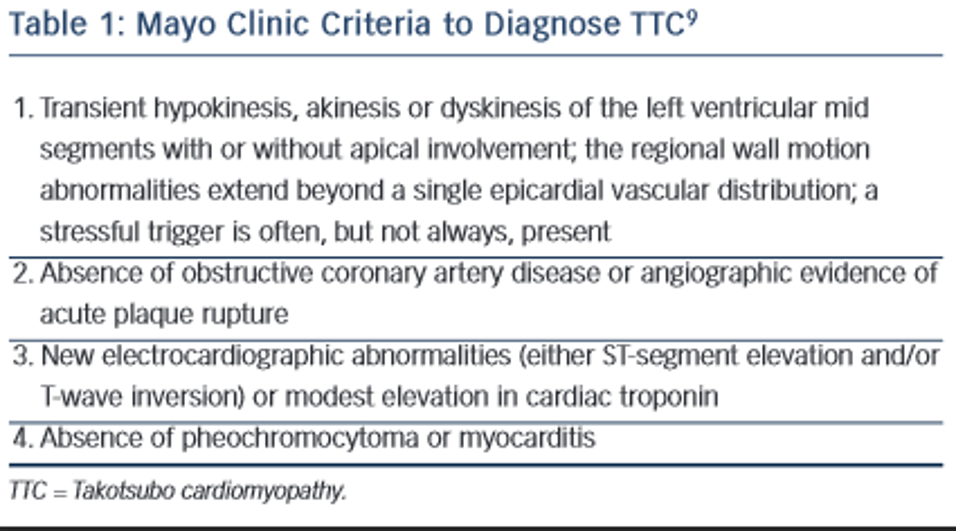
Diagnosis
Mayo Clinic Criteria can help with diagnosis of takotsubo cardiomyopathy.
All four criteria are required for diagnosis.
Echo
- Apical ballooning of LV reflecting regional wall motion abnormalities
- Reduced EF
Treatment
- Conservative, supportive treatment
- Thromboembolism
Treatment recommendations are extrapolated from studies of patients who’ve suffered an MI and subsequently developed intraventricular thrombus- Presence of intraventricular thrombus
- Treat with Vitamin K antagonist (Warfarin) for ~3 months
- In patients with low bleed risk and severe systolic dysfunction (LV EF <30%) and no evidence of intraventricular thrombus
- Can consider prophylaxis with Vitamin K antagonist (Warfarin) until LV dysfunction resolves OR for 3 months (whichever is shorter)
- Presence of intraventricular thrombus
