
We discussed a case about a middle-aged woman with HTN, uncontrolled T2DM, hx of MRSA otitis externa, who presented with subacute myalgias and bilateral leg pain with fevers and chills, found to have MRSA bacteremia and multiple MRSA SSTI / abscesses. Her hospital course was complicated by a drug reaction (rash) to Vancomycin, so she was treated with Daptomycin. Later on, she developed acute hypoxic respiratory failure, peripheral eosinophilia, and found to have acute eosinophilic pneumonia due to Daptomycin.
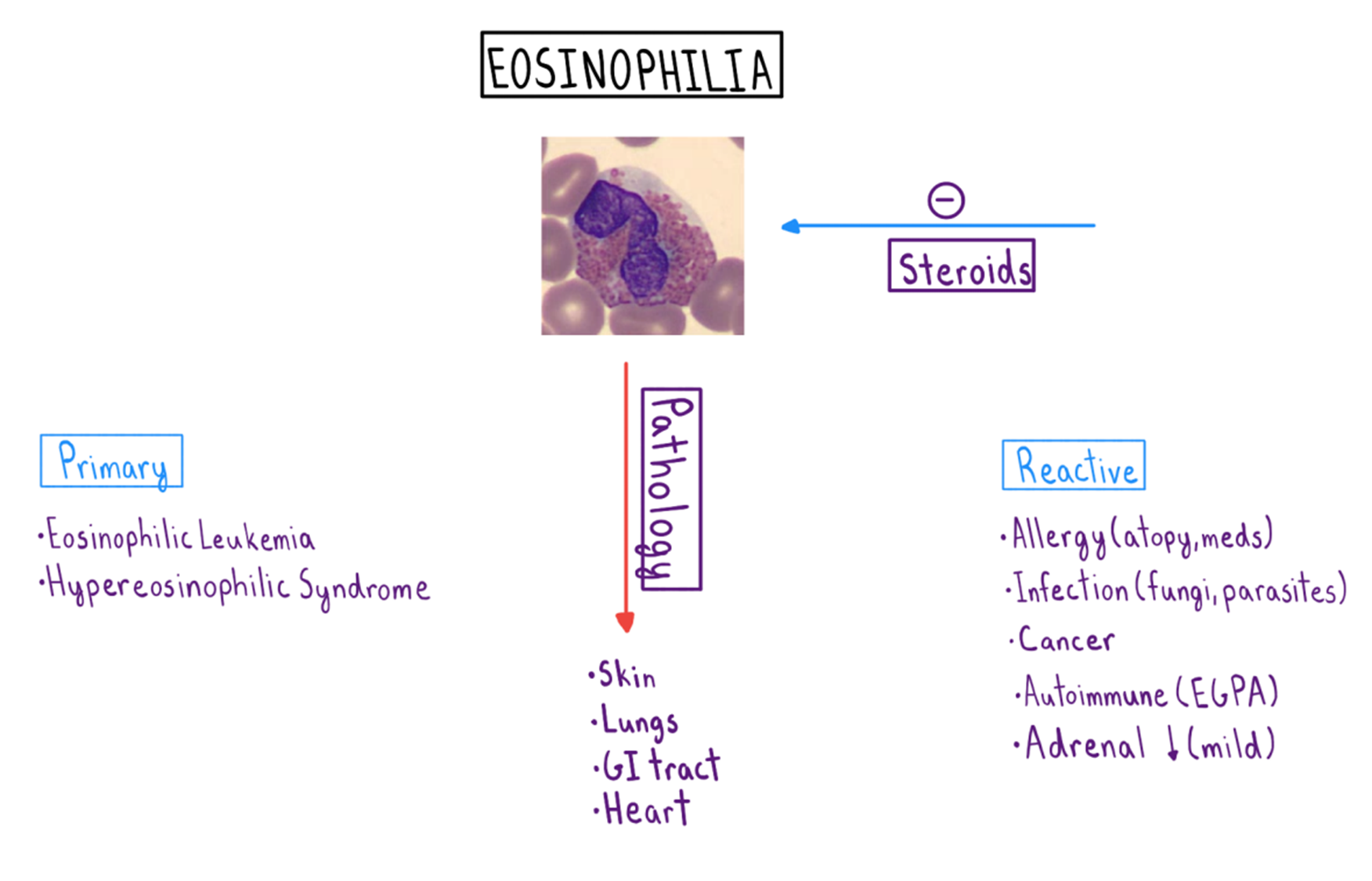
Eosinophilia
Eosinophils can infiltrate into any organ and cause damage
- Peripheral absolute eosinophilia > 500
- Mild: 500-1500
- Moderate: 1500-5000
- Severe: >5000
Eosinophilia Differential
ACUTE Eosinophilic pneumonia
- Febrile illness
- < 7 days of nonproductive cough, dyspnea, and diffuse pulmonary opacities
- Can lead to respiratory failure in hours to short days
- Diagnosed by
- Clinical presentation / symptoms
- Chest imaging
- BAL with ≥ 25% eosinophils
- Note: you may not see peripheral eosinophilia during the early stages of disease
CAUSES OF PULMONARY EOSINOPHILIA
- Toxins (inhalation)
- Cigarette smoking, dust
- Cocaine, meth, marijuana, heroin
- Medications
- NSAIDs
- Antibiotics (e.g. daptomycin, sulfonamides)
- Anticonvulsants (e.g. phenytoin)
- Infections
- Parasite (e.g. strongyloides)
- Fungi (e.g. aspergillus, coccidiodomycosis, cryptococcus)
- Vasculitis (e.g. EGPA)
- Neoplasms (e.g. lung cancers, metastasis)
- Interstitial Lung Disease
MANAGEMENT
- Treat the underlying cause
- Glucocorticoids
REFERENCES
