We discussed a middle aged female with uncontrolled diabetes that presents with profound subacute (5 week history) development of proximal over distal weakness and associated muscle pain. Other symptoms included 1 week of dysphagia to solid>liquid food. Overall, she presented with proximal muscle weakness with absent Babinski sign and 2+ reflexes bilaterally. Her medication included Simvastatin 20qhs. EMG shows myopathic process; ANA 1:160; HMGcoAR Antibody negative, Anti-SRP negative; biopsy showing fibrocellular variation with necrotic fibers within clusters of inflammation most consistent with necrotizing myopathy. CTCAP showed a large mediastinal mass which are diagnosed to be a invasive thymoma. Due to symptoms of dysphagia and probably bulbar involvement, patient was checked for associated myasthenia gravis. Ach Receptor Ab 159 mmol/L and 1:2560 striated muscle antibody IGg titer. Anti MUSK negative. Patient was treated with thymectomy and IVIG followed by rituximab.
We know that this patient was not dealing with a UMN or LMN process but rather a muscular weakness. We discussed framework of proximal muscle weakness, particularly in regards to muscle weakness and neuromuscular weakness.
Differential for muscle weakness:
- Medication
- Toxins
- Electrolyte disturbances
- Deconditioning
- Endocrinopathy
- Critical illness
- Rhabdomyolysis
- Infection
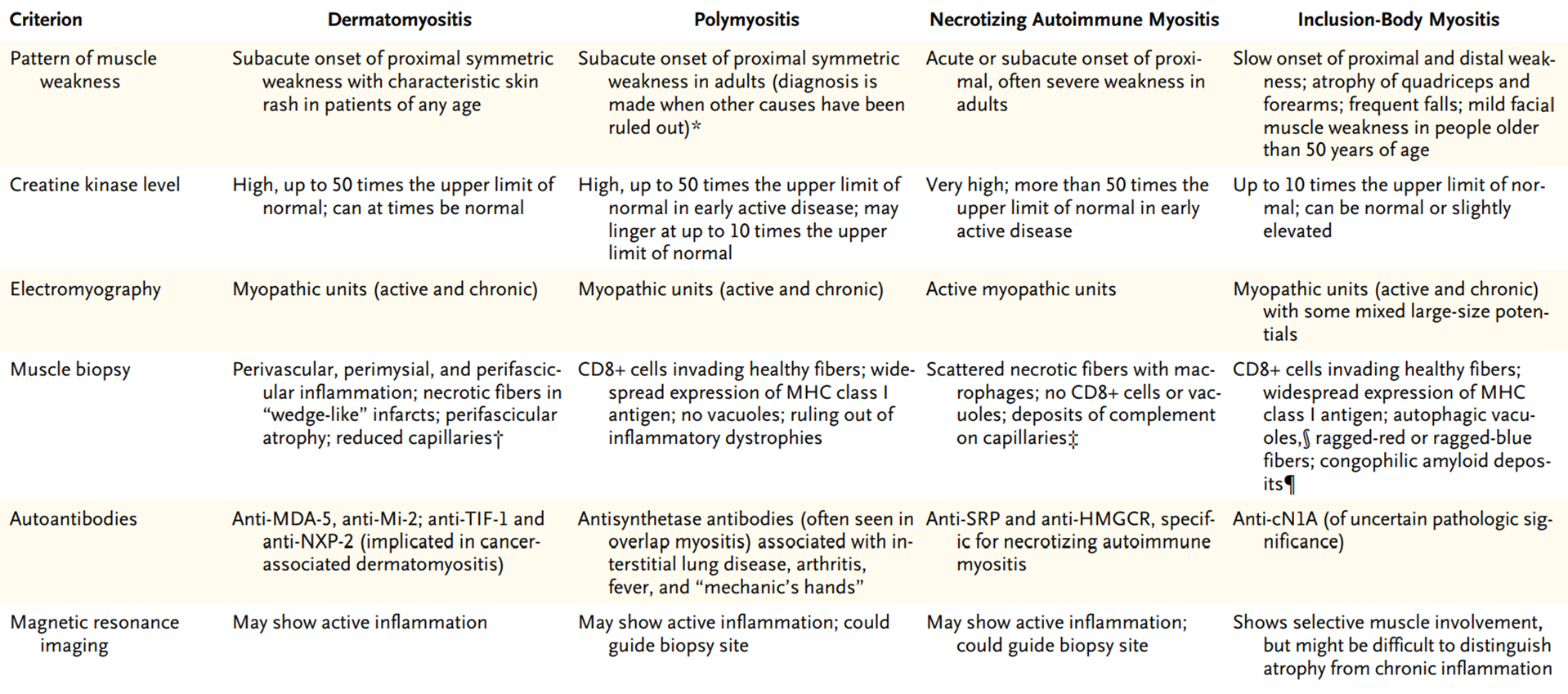
- Inflammatory Myopathy (DM, PM, Inclusion body myositis)
- Muscular Dystrophy
- Metabolic Myopathy