
- Diagnostic Criteria for APLS: Need ONE lab criteria (confirmed 12 weeks apart) and ONE clinical criteria.
- LAB Criteria: B2 Glycoprotein, Anti-Cardiolipin antibody, or lupus anticoagulant (as measured by prolonged DRVVT which does not correct with a mixing study)
- CLINICAL Criteria: Any Thrombosis (venous/arterial) OR fetal loss/miscarriage
- APLS can be a primary disorder or secondary to other disease (usually Lupus)
- Clinical Features of APLS: 50% have prolonged PTT, 20% with livedo reticularis, cardiac valvular disease (MR), 32% DVT, 13% stroke, 7% hemolytic anemia
- Massive PE refers to PE causing hemodynamic instability (SBP < 90) while submassive PE refers to PE causing right heart strain without hypotension
- Right heart strain from PE: Look for signs of right ventricular hypertrophy and dilatation on EKG, Echo. McConnell’s sign on ECHO is RV hypokinesis with apical sparing
Category Archives: Morning Report
Resident Report 11/9 – Rheumatoid Arthritis
Teaching Pearls:
- Average Age 30-55 years old; F:M ratio 3:1
- Symmetric polyarthritis
- Morning stiffness >1 hour that improves with activity
- OA worsens with activity
- Joint Involvement:
- Almost always involves MCP, PIP, wrist, MTP
- Spares the DIP and lumbar spine
- Think of OA with DIP involvement
- Can occasionally affect large joints
- Swan Neck Deformity
- Boutonniere deformity
- Ulnar Deviation
- C1-C2 subluxation (Atlanto-axial instability)
- This specifically can also be seen in Downs syndrome
- Peri-articular osteopenia
- RA is an independent risk factor for pre-mature coronary artery disease
- RA + pancytopenia + splenomegaly = Felty Syndrome
- RA is a systemic disease that can affect multiple organs. Can be a cause for secondary amyloidosis.
- Amyloidosis – deposition disease that clinically affects the kidneys, liver, and heart.
- Kidney – can lead to nephrotic syndrome
- Hepatomegaly
- Restrictive cardiomyopathy
- Thickening of tongue – lateral scalloping seen on exam
- Waxy skin
- Coagulopathy – amyloid protein causes binding to factor X
- Neuropathy
- GI – causing a malabsorptive syndrome
- Diagnosis requires abdominal fat pad biopsy with Congo red stain to check for apple-green birefringence.
Morning Report 11/4 – CREST and Dermatomyositis
Teaching Pearls:
- Clinical Features of CREST syndrome
- Calcinosis of soft tissue, Raynauds phenomenon, Esophageal dysmotility, Sclerodactyl, Telangiectasia
- Diffuse Cutaneous Systemic Sclerosis (dcSS)
- Skin Findings – Extends past elbows and knees from hands and feet, respectively. Can be seen along torso and face/neck
- Antibody – anti-Scl-70
- Pulm manifestation – interstitial lung disease
- Associated with sclerodermal renal crisis
- Not associated with CREST
- Limited Cutaneous Systemic Sclerosis (lcSS)
- Skin Findings – hands/feet, distal to elbows and knees. Face and neck
- Antibody – ANA centromere pattern
- Pulm manifestation – pulmonary hypertension
- Not associated with sclerodermal renal crisis
- Associated with CREST
- Dermatomyositis
- Heliotropic rash, shawls and V sign, gottron’s papules. Mechanic hands
- Classically associated with proximal muscle weakness
- Elevated CK and aldolase.
- Other studies to consider: EMG and muscle biopsy (definitive diagnosis)
- Associated with anti-Jo-1 antibody (anti-synthetase syndrome)
- Higher association with ILD and worse prognosis
- Higher association with malignancy.
- Colon, breast, ovarian, prostate, etc.
- Few case reports have found an association with oropharyngeal dysphagia, and seems to suggest a poor prognosis sign.
- Serologic Studies/Associations
- Anti-centromere pattern of ANA – lcSS
- Anti-dsDNA Ab – SLE
- Anti-smooth muscle Ab – autoimmune hepatitis
- Anti-La/SSB antibody – Sjogrens, neonatal SLE
- Anti-RNP antibody – Mixed connective tissue disease
- Antihistone antibody – drug induced lupus
- Anti-Scl-70 Ab – dcSS
- Anti-Ro/SSA antibody – Sjogrens, neonatal heart block
- c-ANCA – Wegeners granulomatosis
- p-ANCA – Churg Strauss, microscopic polyangitis
- Anti-Jo-1 Ab – dermatomyositis/polymyositis/anti-synthetase syndrome
- Anti-CCP Ab – Rheumatoid arthritis
Morning Report 11/3 – Hyponatremia
Teaching Pearls:
- Can be categorized into the following:
- Hyperosmolar
- Hyperglycemia, mannitol use
- Iso-osmolar
- Hypertriglyceridemia, hyperparaproteinemia
- Hypo-osmolar
- Hyperosmolar
- Hypo-osmolar hyponatremia can be divided into different categories based on volume status:
- Hypovolemic
- GI losses, diuretic use, blood loss
- ↓↓salt/↓H2O
- Urine osm >100mOsm/L
- Urine Na <20 mmol/L
- Euvolemic
- siADH, psychogenic polydipsia, adrenal insufficiency, hypothyroidism, low solute intake (tea toast diet or beer potomania)
- Salt/↑H2O
- siADH
- Urine osm >100mOsm/L
- Urine Na >40 mmol/L
- Psychogenic polydipsia
- Urine osm<100mOsm/L
- Urine Na >20mmol/L
- Hypervolemic
- CHF, nephrotic syndrome, cirrhosis
- ↑Salt/↑↑H2O
- Urine osm >100mOsm/L
- Urine Na <20mmol/L
- Hypovolemic
- Hypothyroidism presents as a hypoosmolar euvolemic hyponatremia.
- Can present with a clinical picture and urine studies similar to siADH
- Can also present as a picture of CHF.
- Often these patients have myxedema coma.
- Theorized that the decreased cardiac output leads to decreased glomerular filtration, leading to poor excretion of free water.
- Adrenal insufficiency commonly presents with hyponatremia, hyperkalemia, and metabolic acidosis.
- Low solute diet (tea toast diet and/or beer potomania)
- Kidneys can dilute urine to as low as 50mOsm/L.
- If intake of solute is very low, then it limits the amount of free water that can be excreted.
- For more teaching points, check out the hyponatremia section on http://www.professorebm.com.
Morning Report 11/2 – Esophageal Variceal (EV) Bleeding
Teaching Pearls:
- Esophageal varices are seen in roughly 50% of patients with cirrhosis.
- About 33% of patients with cirrhosis and esophageal varices will have at least one clinical presentation of esophageal variceal (EV) bleeding.
- Mortality of 15-20% associated with each episode of esophageal bleeding event.
- EV bleeding comprises of 33% of all cirrhosis-related deaths.
- Risk of EV bleeding correlates with size of varices and other characteristics such as nipple sign and red wales sign.
- Pre-primary prophylaxis – Management of cirrhotic patients without esophageal varices
- Management focuses on treating the underlying cause of cirrhosis.
- Screening occurs ~2-3 years.
- Primary Prophylaxis – Management of cirrhotic patients with EV but no clinical history of GI bleed.
- Medical management with beta blockers
- Performed in those with medium-large varices, or small varices with red wales/nipple sign.
- Esophageal band ligation
- Performed in those with large varices
- Continued Monitoring
- Those with small EV without red wales/nipple sign.
- Medical management with beta blockers
- Immediate interventions to consider in patients with suspected EV bleeding:
- At least 2 large bore PIVs (16 or 18G) or central line
- Fluid resuscitation
- Type and screen blood
- Monitor hemodynamics
- Start protonix (bolus and gtt) and octreotide (bolus and gtt)
- Start ceftriaxone for SBP prophylaxis
- Pantoprazole
- PPI will increase the pH of the gastric lumen to 5-6 from 1-2.
- pH changes help with improving clot formation
- Octreotide
- Works by inhibiting endogenous substances – leads to splanchnic vasoconstriction, decreasing portal flow, leading to decreased portal pressures.
- SBP Prophylaxis Conditions
- History of SBP
- Cirrhosis with GI bleed
- Ascitic TP <1
- Management of gastric varices differ from esophageal varices.
- Cyanoacrylate injection and/or TIPS
Morning Report 10/28 – PFTs
Teaching Pearls:
- FEV1/FVC Ratio <0.7 suggestive of obstructive parenchymal disease
- DLCO – ability for gas to diffuse across alveolar capillary membrane. CO (inhaled) – CO (exhaled). CO has a high affinity for Hb. If CO (exhaled) is higher than expected, DLCO is low and this is suggestive of diffusion problem.
- False Positive
- Anemia
- Pulmonary hypertension
- False Negative
- Pulmonary hemorrhage
- False Positive
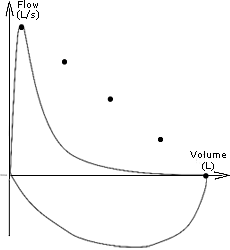
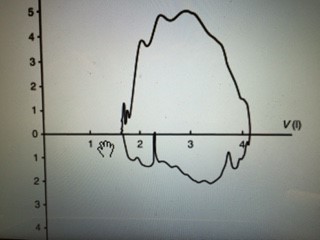
- Pulmonary Function Tests
FEV1 FVC FEV1/FVC DLCO TLC RV F-V Emphysema Decrease Decrease/No change <70% Decrease Normal/increase Normal/increase C Chronic Bronchitis Decrease Decrease/No change <70% Normal Normal/increase Normal/increase C ILD Normal/Decrease Normal/Decrease Normal/Increase Decrease Decrease Decrease A Tracheal stenosis Decrease Decrease/normal Decrease Normal Normal Normal B Resp muscle weakness Decrease Decrease Normal Normal Decrease Increase D A.

B.

- C.

- D.



10/27/15 Morning Report SLE
Teaching Pearls:
- ANA negative lupus, check SSA/SSB which are associated with neonatal lupus and congenital heart block
- ANA positive in 99% of patients with lupus, but low specificity
- double stranded DNA antibodies are used to monitor disease severity in lupus
- check C3, C4, and double stranded DNA to work up possible lupus flare
- Drug induced lupus: Look for positive ANA and anti-histone antibodies. Also look for exposure to procainamide, hydralazine, chlorpromazine, PTU, phenytoin, minocycline, and TNF inhibitors.
| Steroid | Duration | Equivalent Dosing |
| Dexamethasone | Long-acting | 1 mg |
| Methylprednisolone | Intermediate-acting | 4 mg |
| Prednisone | Intermediate-acting | 5 mg |
| Hydrocortisone | Short-acting | 20 mg |
10/22/15 Morning Report Hyperthyroidism
- Pathophysiology of T4 secretion: TSH secreted in the anterior pituitary and stimulates the TSH receptor in the thyroid to secrete thyroid hormone
- Clinical presentation of Hyperthyroidism: Hyperdefecation (not diarrhea), osteoporosis, oligomenorrhea in pre-menopausal females, hair changes, palpitations, arrhythmias
- Etiologies of hyperthyroidism
- Grave’s Disease (most common cause of hyperthyroidism)
- Destructive thyroiditis (subacute, silent, postpartum)
- Multinodular Goiter/Toxic Adenoma
- Medication-induced (amiodarone, lithium, IFN-a, etc)
- Factitious
- Antibodies
- Anti-TPO and anti-thyroglobulin Ab seen with Hashimoto’s Disease (hypothyroidism)
- TSI (thyroid stimulating immunoglobulin) and TBII associated with Graves Disease.
- TSI binds to TSH receptors on thyroid gland, stimulating production of thyroid hormone.
- TSI also binds to TSH receptors located on fibroblasts, stimulating proliferation and glycosaminoglycan production in retro-orbital space.
- Clinical Presentation specific to Graves include pretibial myxedema (5% patients with Graves), exophthalmos (25% of patients with Graves)
- Work-up of Hyperthyroidism
- If evidence for Graves Disease, then GD likely diagnosis.
- Evidence of nodules on physical Exam:
- If None: Perform RAI uptake scan and antibody studies.
- If increased uptake, elevated thyroid hormone due to over-synthesis
- If diffuse uptake, think Graves Disease
- If patchy uptake, think toxic multinodular goiter
- If decreased uptake, think of factitious or destructive causes (subacute, silent, postpartum.
- If increased uptake, elevated thyroid hormone due to over-synthesis
- If Present: Get RAIU scan and thyroid ultrasound to distinguish TNG vs TA and/or evidence of cold nodules. Check for any concerning factors for thyroid cancer.
- If None: Perform RAI uptake scan and antibody studies.
- Thyroglobulin: Precursor to thyroid hormone production. Combined with iodine to produce T4.
- May be used to differentiate factitious vs destructive thyroiditis, surveillance for thyroid cancer.
- Treatment Options:
- Thionamides – Methimazole versus PTU
- Watch for drug rash and/or agranulocytosis
- Radioactive iodine ablation
- Do not use in patients with Graves Disease with severe ophthalmopathy as this can worsen symptoms.
- Surgery
- Thionamides – Methimazole versus PTU
| Grave’s Disease | Multinodular Goiter | Subacute Thyroiditis | |
| Clinical Course/Exam
|
Exophthalmos
Pre-tibial Myxedema |
Hyperthyroid symptoms
Palpable nodules |
Preceded by URI sx, Pain around the neck, pain with palpation, initially hyperthyroid (6 weeks) but progresses to hypothyroid (6 weeks), then normalizes |
| Diagnosis Tests
|
Low TSH
High Free T4 TSI RAIU |
TSH/T4
RAI Thyroid US |
TSH, Free T4
RAI – low uptake Thyroid US – diffuse enlargement |
| Treatment
|
PTU
Methimazole (don’t use in 1st trimester of pregnancy). Watch for agranulocytosis. RAIA, then will require Surgical. Don’t use RAIA for patients with exophthalmos. |
If compressive sx (dysphagia, etc) then surgery
If no compressive symptoms, can treat with RAIU. Toxic patients can also be treated with thionamides |
NSAIDS, supportive
Then Prednisone if poor response Symptomatic treatment, such as propranolol or beta blockers Thionamides not indicated |
Intern Report 10/20 – Bloody Diarrhea
Teaching Pearls
- Duration of Diarrhea
- Acute < 14 days
- Chronic >4 weeks
- Types of Diarrhea
- Secretory
- Stool osmole gap <50
- Osmotic
- Stool osmole gap >100
- Inflammatory
- Evidence of blood and/or mucoid stools
- Malabsorption
- Protein-losing enteropathy
- CHO malabsorption
- Fat malabsorption
- Secretory
- Bacterial Causes of Blood Diarrhea
Source Presentation Complications Treatment STEC (EHEC) Uncooked hamburger meat. Fecal-oral route
Abd pain with bloody diarrhea +/- fever HUS No antibiotics indicated; supportive care Shigella Shellfish, fecal oral route Dysentery (bloody mucoid stools), tenesmus, fever, abdominal pain Reiters Disease Flouroquinolone; 3rd generation cephalosporin Salmonella Undercooked raw eggs, chicken, fruits Fever, abdominal pain, occult/overt bleeding Bacteremia, aortitis, osteomyelitis in those with sickle cell disease Only treat when symptoms are severe Campylobacter Poultry Occult bleeding Reiters disease, Guillain-Barre Syndrome Treat only if severe with macrolides
10/17/15 – Valley Residents Present at ACP in San Francisco!
A shout out to our poster presenters and brave Jeopardy Team! It wouldn’t have been possible without all our housestaff who graciously covered our presenters – thank you very much! Saloni, Courtney, and Joe Li advanced to the finals in the poster competition. Three fascinating ID cases (cutaneous blastomycosis, rat bite fever, and pseudallescheria boydii) which is testament to all the cool ID we see here at Valley!


{kind=link}