
Indications for CT before LP:
- >60 years old
- Immunocompromised state
- History of CNS disease (mass lesion, stroke, focal infection)
- Seizure within 1 week of presentation
- Altered consciousness / focal neurological deficit
* Patients with suspected meningitis without the above findings are good candidates for LP without CT given their low risk for herniation.
| CSF Studies: | Normal | Bacterial Meningitis | Viral Meningitis | Fungal/TB Meningitis |
| Opening Pressure (cm H20) | <15 | ↑ | Normal/↑ | Normal/↑ |
| Protein (mg/dL) | 15-45 | ↑ | Normal/↑ | ↑ |
| Glucose (mg/dL) | 40-70 | ↓ | Normal | ↓ |
| WBC Count (uL) | 0-8 | ↑↑ (>1000) | ↑ (50-300) | ↑ |
| WBC Differential | Normal | >80% PMNs | >50% Lymphs, <20% PMNs | 50-80% Lymphs |
Common Signs/Symptoms:
- Patient’s often present soon after onset of symptoms ~ 24 hours (range 1 hour – 14 days)
Classic Triad:
- Fever (95-77% at presentation)
- Nuchal Rigidity (94-83% at presentation)
- Altered Mental Status (83-78% at presentation)
- *Headache (94-79% at presentation)
*One review of 696 cases of community-acquired bacterial; only 44% had clinical triad, although almost all (95%) had at least 2 of 4 symptoms.
Laboratory Findings (besides CSF):
- Routine blood work is often unrevealing, but leukocytosis can be present
- Serum chemistry may reveal an AG metabolic acidosis or hyponatremia (30% in one study)
- Blood cultures are often positive (50-90% of patients) and can help guide therapy
Common Pathogens:
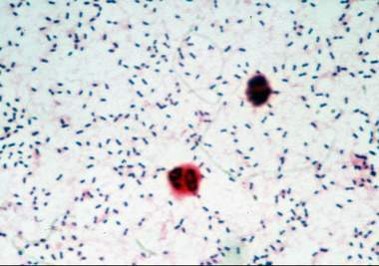
- Streptococcus pneumoniae (71%)
- Neisseria meningitidis (12%)
- Group B Streptococcus (7%)
- Haemophilus influenza (6%)
- Listeria moncytogenes (4%)
* Percentages based on CDC data of 1083 cases of bacterial meningitis from 2003-2007
Treatment for Suspected Bacterial Meningitis:
- Empiric therapy should be directed at the most likely bacteria and must be started without delay
Typical empiric regimen:
- 3rd generation cephalosporin (Ceftriaxone 2 g IV Q12H or Cefotaxime 2 g IV Q6H)
- Vancomycin 15-20 mg/kg IV Q12H ~ goal trough 15-20 mcg/mL
- Ampicillin in patients > 50 years old
Indications for Steroids:
- Used in attempt to diminish the rate of neurological complications (seizures, hearing loss, cranial nerve deficits, etc.)
- European studies showed a decreased mortality (7% versus 15% with placebo)
- Only indicated for patients with suspected/confirmed S. pneumoniae
- 15 minutes before administration of antimicrobial agents and continued for full course (0.15 mg/kg Q6H for 4 days) in suspected/confirmed pneumococcal meningitis
