Etiologies of a PROLONGED Qtc (not an exhaustive list)
Remember that many LOW electrolytes can lead to prolonged Qtc increasing risk of arrhythmias (usually Torsades)
–Drugs (large category, includes anti-psychotics, anti-arrhythmics,TCA, anti-histamines)
-HYPOkalemia
-HYPOmagnesemia
-HYPOcalcemia
-HYPOthermia
-Congenital (eg: long QT syndrome)
What can cause HYPOcalcemia?
-HYPOparathyroidism (PTH controls calcium and phosphorus homeostasis)
-HYPOproteinemia (Pearl: always check albumin with calcium unless you are checking ionized calcium!~0.8 increase in calcium for every 1.0 decrease in albumin from 4.0)
–Renal disease (remember that the kidney makes activated Vit D with 1 alpha hydroxylase and Vit D absorbs calcium from the gut)
-Vit D deficiency (cannot absorb calcium)
-Hyperphosphatemia (binds calcium and lowers serum levels, is the etiology of hypocalcemia in Rhabdo and TLS)
-Acute Pancreatitis
-Chelation (eg: after being given Citrate/EDTA/Foscarnet)
-Hypomagnesemia (Mg needed for PTH activity)
-Hungry bone syndrome (seen after parathyroid surgery for elevated PTH where bones start sequestering the calcium levels in the serum)
Clinical manifestations of HYPOcalcemia
Remember CATS mnemonic!

NEUROMUSCULAR IRRITABILITY
-Parethesias
-Tetany
-Trousseau’s sign-carpopedal spasm seen when inflating BP in upper arm above systolic pressure (highly sensitive and specific!)
-Chvostek’s sign- facial twitching in response to tapping over facial nerve (absent in one third of patients with hypocalcemia, and seen in 10 % of patients with normal calcium levels!)-Bronchospasm/Laryngospasm
CARDIAC
-Prolonged Qtc, Arrhythymia
-Hypotension, HF
NEUROLOGIC
-Seizures
-Extra pyramidal symptoms (eg: Parkinsonism)
-Irritability, depression, personality changes
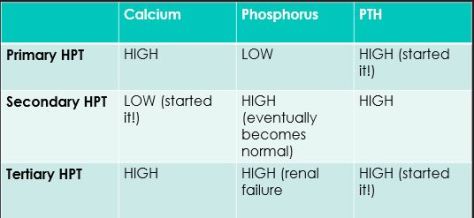
PRIMARY vs. SECONDARY vs. TERTIARY HPT
Where does the problem start?
Primary– Elevated PTH is the problem leading to high Ca, low Phos
Secondary-LOW calcium is the problem leading to elevated PTH
Tertiary-PTH is again the problem but it is functioning autonomously due to uncontrolled secondary PTH or post-renal transplant so calcium is elevated but phosphorus still elevated due to renal failure.