
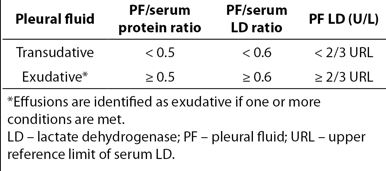
Remember Light’s Criteria is SENSITIVE for picking up EXUDATES but mis-classifies ~25% transudative effusions as exudative!
-You only need to have ONE of Light’s criteria to call it an Exudate!
TRANSUDATE
Remember the top 3 but there is an extensive list…
–CHF (most common)
-Hepatic hydro-thorax from cirrhosis
-Nephrotic syndrome
EXUDATE
Remember the top 3 but also has an extensive list…
-Malignancy
-Pneumonia
-Tb
What percentage of patients with bacterial PNA get an associated effusion?
>40 % and up to 60 % with pneumococcal PNA, and can be either uncomplicated, complicated, or empyema
Uncomplicated parapneumonic effusion
-Resolves with antibiotic treatment of PNA
-On CXR, must be free-flowing and <10 mm
-Very low risk, does not need drainage
Complicated parapneumonic effusion
-Small/Mod in size, >10 mm but <1/2 hemithorax
-Negative gram stain/culture, pH>7.20
-May need drainage based on clinical status
Complicated parapneumonic effusion (second type)
-Large >1/2 hemithorax, LOCULATED, thickened parietal pleura (high risk if thickened parietal pleura, suspect Empyema)
-Positive culture or gram stain OR
-pH<7.20
-MUST drain effusion, moderate risk
EMPYEMA!
-defined as PURULENT appearance of pleural fluid OR
–pH <7.20 (don’t forget to order pH and keep it on ice!)
-If ether of these exist, MUST drain effusion, highest risk, usually with tube thoracostomy (chest tube)
Treatment
-Empiric therapy should cover Gram + (eg: Staph, Strep), and Anaerobes (eg: Fusobacterium, Bacteriodes)
-Empyema is treated with 4-6 weeks of antibiotic treatment

