
Remember that Acute Cholangitis is a medical emergency that must be recognized and treated emergently!
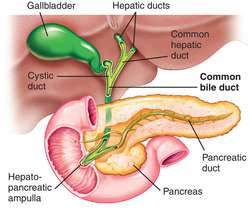
CBD diameter
Remember that CBD diameter can be a clue to biliary obstruction
-95 % of normal patients have a CBD < 6 mm
-Can increase with age, usually upper limit corresponds to decade of life (70 year old upper limit of ~ 7 mm
-Can see CBD up to 10 mm if post-cholecystectomy!
If you suspect choledocholithiasis, the ASGE guidelines can help you decide whether you should do an MRCP or an ERCP
-Remember if you have any very strong predictors (see below), you should go directly to an ERCP!
Very strong predictors of choledocholithiasis
-CBD stone seen on trans abdominal ultrasound
-Bilirubin>4 mg/dl
-Clinical ascending cholangitis


MRCP vs. ERCP
MRCP=diagnostic modality, NO contrast given, excellent sensitivity to evaluate for choledocholithasisis (90-100%)
ERCP=diagnostic and therapeutic modality, invasive (have to be in prone position!), risk of post-ERCP pancreatitis
Four main etiologies of biliary obstruction
–Choledocholithasis (MCC)
-Biliary strictures
-Malignancies
-Biliary stent complication (eg: migration)
Etiology
GUT FLORA
-E.Coli (most common), Klebsiella, Enterobacter, Enterococcus, and Anaerobes (less common alone)
Key Clinical manifestations and lab findings for cholangitis and which ones are most common
-Fever (95 %)
-RUQ pain (90 %)
-Jaundice (80 %)
Charcot’s Triad=>Fever, RUQ, Jaundice
(+) Hypotension, Confusion, Leukocytosis, Cholestatic jaundice.
Treatment for empiric coverage for cholangitis
-Beta Lacam/Beta Lactamase inhibitor
-Flouroquinolone + Flagyl
-Carbapenem
Management for cholangitis in addition to antibiotics
-ERCP for source control, treatment of sepsis, and cholecystectomy
