
Calcium correction:
- Corrected Calcium = (0.8 (normal albumin – patient’s albumin)) + Ca2+
- Check an ionized (free) calcium
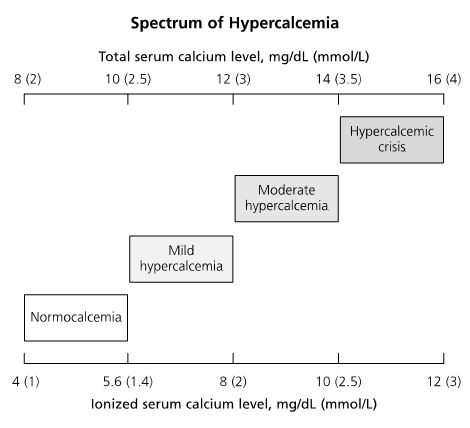
Interpreting the degree of hypercalcemia:
- Normal (8-10 mg/dL)
- Mild hypercalcemia (10-12 mg/dL)
- Moderate hypercalcemia (12-14 mg/dL)
- Hypercalcemic crisis (>14 mg/dL)
Remember the clinical manifestations of hypercalcemia: “stones, bones, abdominal groans, thrones, and psychiatric overtones”

ECG in hypercalcemia:
- the main ECG abnormality with hypercalcemia is shortening of the QT interval
- in severe hypercalcemia, Osborn waves (J waves) may be seen
3 Main hormones involved in calcium homeostasis:

Etiologies of Hypercalcemia:

| Pathophysiology/ Causes | Calcium Level | PTH Level | 1, 25-vitamin D | Phosphorous | |
| Primary Hyperparathyroidism | Overproduction of PTH, 85% due to single adenoma | ↑ | ↑ | ↑ | ↓ |
| Secondary Hyperparathyroidism | Overproduction of PTH, commonly due to chronic renal failure | ↔ or ↓ | ↑ | ↓ | ↔ or ↑ |
| Tertiary Hyperparathyroidism | Overproduction of PTH, usually by autonomous hypersecretion of PTH | ↑ | ↑↑ | ↓ | ↑ |

Treatment of Hypercalcemia:
- Any symptomatic patient with a calcium level > 12 mg/dL
- Any patient with calcium level > 14 mg/dL
Treatment options:
- IVF (NS) – enhances filtration/excretion of Ca2+; tailored towards urine output ~ 200 mL/hr
- Loop Diuretics (Furosemide) – inhibits calcium reabsorption in the distal tubule; only use one volume status restored
- Bisphosphonate – inhibits osteoclast action/bone reabsorption; indicated in hypercalcemia of malignancy; avoid in renal failure
- Calcitonin – inhibits bone resorption and promotes Ca2+ excretion; recommended for severe cases after IV hydration
- Glucocorticoids – inhibits vitamin D conversion to calcitriol; used for vitamin D intoxication, hematologic malignancies, and granulomatous disease
- Dialysis – used for cases of resistant, life-threatening hypercalcemia

One thought on “AM Report 12/20/2016: Hypercalcemia”