
Today, we discussed the case of a middle-aged woman with no significant medical history who presented to PCP with a month of nausea, vomiting, weakness, and 30 pound weight loss, found to have severe hypercalcemia likely secondary to a granulomatous disease. Final diagnosis pending biopsy results.
Clinical Pearls
- The first step in working up hypercalcemia is correcting for albumin. Keep in mind that patients with hypoalbuminemia may have a falsely low serum calcium level. Conversely, patients with multiple myeloma who have a high paraprotein serum concentration may have a falsely elevated total serum calcium level. When in doubt, check an ionized serum calcium to confirm true hypercalcemia.
- Think of hypercalcemia in two broad categories of PTH dependent disorders and PTH independent disorders (see below).
- 25-OH vitamin D has a long half life and is the best laboratory test to determine adequate nutritional intake of vitamin D. In contrast, 1,25OH vitamin D has a short half life.
Calcium homeostasis:
- Remember that bone is the largest reservoir of calcium in the body.

Source: this NEJM case
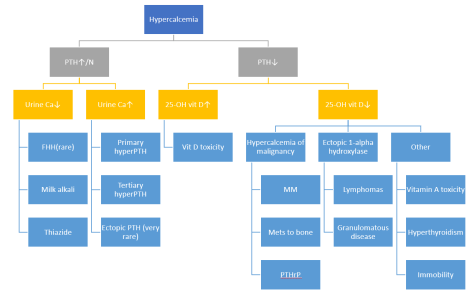
Work up of hypercalcemia
- Remember to confirm true hypercalcemia by correcting for albumin and/or measuring ionized calcium for people with conditions such as multiple myeloma who may have a falsely elevated total serum calcium due to increased paraprotein binding.
- Check out this super awesome previous post on hypercalcemia on our blog for more details. Here is the simplified diagnostic algorithm we went over today:
Treatment
- Ca <12
- No treatment if asymptomatic
- Avoid exacerbating factors
- Ca 12-14
- If chronic/asymptomatic ⇒ same treatment as Ca <12
- If acute/symptomatic ⇒ same treatment as Ca 14-18
- Ca 14-18
- IVF – LOTS!
- Lasix only if the patient has concurrent renal/heart failure
- Calcitonin
- Bisphosphobates
- Zoledronic acid >> pamidronate for patients with malignancy
- Do not use in patients with Cr >4.5
- Denosumab (RANKL) if refractory to zoledronic acid or in patients with severe renal impairment
- Ca >18
- Same treatment as Ca 14-18 PLUS
- Hemodialysis
Treatment options: (table adapted from UpToDate)

* Only used in patients with renal insufficiency or heart failure, judicious use of loop diuretics may be required to prevent fluid overload during saline hydration.
Vitamin D metabolism
- Remember the following simplified pathway of vitamin D metabolism

Source: Hepatitis B Foundation
- 25-OH vitamin D has a long half-life and the best laboratory test to perform to determine adequacy of nutritional intake
- In work up of hypercalcemia, it is also important to check 1,25-dihydroxyvitamin D levels. Why?
- Remember that 1-alpha hydroxylase is an enzyme in the kidney that converts 25-OH vitamin D into its metabolically active form ⇒ 1,25-dihydroxyvitamin D
- It turns out that in certain granulomatous diseases and lymphoma, activated monocytes in affected tissues start to express 1-alpha hydroxylase as well, resulting in overproduction of 1,25-dihydroxyvitamin D.
- So, in work up of hypercalcemia that is PTH-independent, if you notice elevated 1,25-dihydroxyvitamin D with normal 25-OH vitamin D levels, suspect granulomatous disease or lymphoma causing exogenous 1,25-dihydroxyvitamin D production.
