
- Risk Factors
- Mean intake of 100g/day for 10-20 years
- Standard drink of ETOH = 14g pure alcohol
- 12oz beer
- 5oz wine
- 5 oz of 80 proof liquor (“Shot”)
- Standard drink of ETOH = 14g pure alcohol
- Binge drinking
- Men = 5 drinks in 1 sitting
- Women = 4 drinks
- Mean intake of 100g/day for 10-20 years
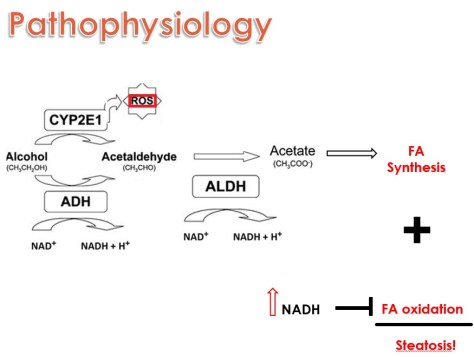
- Pathophysiology
- Standard alcohol metabolism in cells
- Alcohol dehydrogenase (ADH) plus cytochrome P-450 2E1 (CYP2E1) convert ethanol into acetaldehyde which is then converted to acetate
- CYP2E1 releases reactive oxygen species leading to inflammation
- NAD+ is used as oxidizing agent for ADH and is converted to NADH
- Excess alcohol creates an imbalance of NAD/NADH
- Excess NADH decreases oxidation of fatty acid oxidation
- While acetate increases fatty acid synthesis
- Both leading to steatosis
- Both leading to steatosis
- Standard alcohol metabolism in cells
- Presentation
- Pts often present between 40-50 years of age
- Classic presenting features
- Jaundice
- Scleral icterus
- Anorexia
- Fever
- Tender RUQ
- Hepatomegaly
- Abdominal distention due to ascites
- Hepatic encephalopathy
- Bruit can be appreciated over the liver due to increased hepatic blood flow
Labs
- LFTs
- Moderate elevations of AST and ALT
- Usually less than 300, rarely higher than 500
- AST:ALT ratio >2
- ALT is less due to alcohol induced deficiency of Pyridoxal 5-phosphate, which is a coenzyme of ALT. Thus the ratio reflects the failure to appropriately increase the ALT, rather than an inappropriate increase in AST.
- Elevated Tbili and Dbili
- Moderate elevations of AST and ALT
- CBC
- Leukocytosis (usually <20) with a neutrophil predominance
- Extreme Leukemoid reaction (>50) is associated with a very poor prognosis.
- Macrocytosis
- Reflective of poor nutritional status
- Thrombocytopenia
- Leukocytosis (usually <20) with a neutrophil predominance
-
- Coags
- Elevated INR
- Coags
- Imaging (show pics!)
- 1st choice: Abdominal ultrasound
- It’s quick, easy, and relatively cheap
- Will help rule out Budd-Chiari, abscess, obstruction, or neoplasm
- Will show fatty changes in liver vs underlying cirrhosis
- 1st choice: Abdominal ultrasound
- Maddrey Discriminant Function
- DF >32 signifies severe alc hep and is associated with high short-term mortality
- May benefit from glucocorticoid therapy
- DF >32 signifies severe alc hep and is associated with high short-term mortality
- Treatment
- 3 main things
- Alcohol cessation
- Nutritional support
- Steroids
- Contraindicated for:
- GI Bleed
- Infection
- Renal failure
- Pancreatitis
- Check Lille Score on day 7 to evaluate response
- >.45 is associated with 6-month survival of 25% –> ok to stop steroids
- <.45 is associated with 85% survival
- Contraindicated for:
- Pentoxyfilline –> little evidence!
- The Steroids or Pentoxifylline for Alcoholic Hepatitis (STOPAH) trial was just published in the New England Journal in 2015.
- They found a significant 28 day mortality benefit for prednisolone with an odds ratio of .61.
- However, the mortality benefit was lost at 90 days and 1 year
- On the other hand, pentoxifylline did not improve survival compared to placebo
- They found a significant 28 day mortality benefit for prednisolone with an odds ratio of .61.
- The Steroids or Pentoxifylline for Alcoholic Hepatitis (STOPAH) trial was just published in the New England Journal in 2015.
- 3 main things
