
Thank you Naina for presenting the case of an elderly man with 20 packyear smoking history presenting with acute onset of dyspnea and scant hemoptysis, found to have new onset A fib and L heart failure secondary to severe mitral regurgitation resulting from papillary muscle rupture!
Clinical Pearls
- In patients with severe mitral regurgitation (MR) and a normal L atrium size, think about acute causes of MR. TEE is often indicated to better visualize the valve structure and determine need for operative intervention.
- MR can be caused by papillary muscle rupture, especially 3-7 days post MI. Other etiologies of rupture include endocarditis and myxomatous valve degeneration.
- Patients with rupture present with acute onset hypotension, pulmonary edema, and a hyperactive precordium. A systolic murmur is not always present!
- Treatment:
- Aggressive afterload reduction AND
- Surgery (high mortality rate 20-25%)
Atrial Fribrillation
Categories:
- Paroxysmal (terminates within 7 days)
- Persistent (>7 days)
- Long-standing persistent (>1 year)
Differential for new onset A fib: (PIRATES!)
- Pulmonary (OSA, PE, COPD, PNA)
- Ischemia/infarction/CAD*
- Rheumatic heart disease/mitral regurgitation
- Alcohol/anemia (high output failure
- Thyrotoxicosis/toxins (stimulants)
- Electrolytes/endocarditis
- Sepsis/sick sinus syndrome
- Other: HTN*, congenital heart disease, previous cardiac surgery, viral infections
* Most common causes in the US.
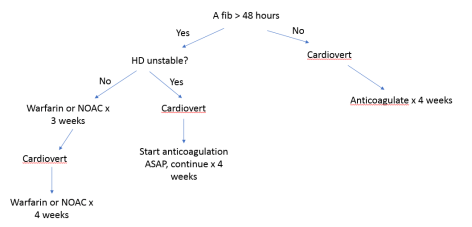
Treatment:
- Rate control (preferred method based on AFFIRM and RACE trials)
- Beta blockers
- Calcium channel blockers ⇒ contraindicated in decompensated heart failure
- Digoxin ⇒ avoid use in renal failure, hypokalemia, hypomagnesemia, or hypercalcemia
- Amiodarone
- Rhythm control
- Methods:
- Chemical (~30% success rate)
- Class III (amiodarone, sotalol, ibutilide)
- Electrical (synchronized to QRS, ~80% success rate)
- Chemical (~30% success rate)
- Preferred modality in
- Hemodynamically unstable
- Young patient (age <65) or good functional status
- Early in natural history of disease
- Failure of rate control agents
- Heart failure
- Methods:
Complications post MI:

Figure from article by Reed et al. Lancet. 2017.
Papillary muscle rupture:
- Posteromedial muscle is 6-12x more likely because blood supply is through PDA only. Anterolateral muscle receives dual supply from LAD and LCx.
- Clinical presentation
- Acute onset hypotension, pulmonary edema
- Hyperactive precordium
- Mid, late, or holosystolic murmur with widespread radiation (though many have no murmur!)
- Diagnosis requires TTE/TEE
- Treatment:
- Aggressive afterload reduction
- Urgent/emergent surgical intervention (20-25% mortality)
