
An elderly lady presented to the ED with what seems like orthostatic hypotension… Found to be anemic but otherwise no complaints. Her lab work incidentally revealed anemia, low anion gap, and grossly elevated protein gap (11.3), but otherwise nothing else! What’s going on?
Low Anion Gap:
- Definition: Less than 3
- Most common cause: Lab error!
- Other causes: hypoalbuminemia, severe hyperchloremic metabolic acidosis, lithium intoxication, hyperklameia, hypercalcemia, hypermagnesemia…
- Could also be a hint of presence of weird proteins!
Elevated Protein Gap:
- Recall: Protein gap = Serum Protein – Serum Albumin, greater than 4 = elevated
- Non-specific finding but can be caused by any processes that leads to an increase in non-albumin serum proteins, again could be a hint of presence of weird proteins??
Her peripheral blood smear revealed presence of Rouleaux, which is another hint of elevated levels of serum protein (but we already know that!). Hematology was consulted and the top differential at this point is some sort of gammopathy, with Waldenstrom’s Macroglobulinemia and Multiple Myeloma highest on the possibilities:
| MM | Waldenstrom macroglobulinemia | |
| Presentation | Fatigue, anemia, Bsx, bone pain, rarely has hyperviscosity | Fatigue, anemia, Bsx, neurologic sx (hyperviscosity, more common) |
| M-protein | IgG, IgM is very very rare | IgM |
| Bone-marrow | >10% clonal plasma cells, CD56 positive | Lymphoplasmacytic infiltration, CD 19, CD 20 positive. CD56 negative. |
SPEP revealed monoclonal IgG spike, and bone marrow revealed > 60% plasmacytosis, hence pt has multiple myeloma!
Do not be tricked! If SPEP revealed polyclonal protein elevation, it could be due to a systemic inflammatory process or infection (Hep C, HIV for instance!)
Multiple Myeloma
- Diagnosis
- SPEP/UPEP for immune proteins
- Smar: > 50% Rouleaux formation, seen with elevated serum proteins
- BM Bx: Looks at % of plasma cells in the marrow, also can do cytogenetics
- Xrays: Lytic lesions (Bone Survey, not a bone scan)
- Other: Cr, calcium, albumin, beta 2 microglobulin (levels help determine staging with prognostic differences)
- > 60% plasma cells on BM has poor prognosis
- UA picks up albumin, NOT light chains
- Light chain: Normal kappa/Lambda FLC ratio is 0.26 – 1.65, MM would have one that’s grossly elevated
- MM Presentation
- Almost all pts will have M-protein spike
- 73% with anemia, 66% with lytic bone lesions, 29% with renal insufficiency.
- Fatigue and normocytic anemia are common findings, blood smear might reveal rouleaux.
- Might cause pancytopenia
- MM Types: based on the kind of abnrl protein
- IgG: 55% of the time, followed by IgA (25%), least common is IgM (0.5%). 20% are light chains only, lacking expression of the immunoglobulin heavy chain.
- Cytogenetics determine high risk vs standard risk myeloma
- High risk = Del 17P, t(14; 16), t(14;20) on FISH
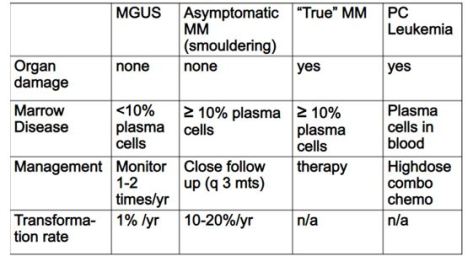
- Management:
- Smouldering: Watch
- Active: treat
- Chemo: 3 drug regimen preferred
- VRd: Bortezomib, lenalidomide, dexamethasone
- VCd/CyBorD: Bortezomib, cyclophosphamide, dexamethasone
- VTd: Bortezomib, thalidomide, dex
- Hematopoietic cell transplantation (HCT): High dose chemo followed by autologous HCT is standard of care if eligible.
- US: case by case, but if pt meets one of the following, they are not eligible for transplant:
- Age > 77
- Cirrhosis
- Poor performance status
- NYHA 3-4
- Chemo: 3 drug regimen preferred
