
Thanks to Joe for presenting the case of an elderly man presenting with subacute onset of AMS, vision changes, and ataxia, found to have creutzfeldt jakob disease (CJD).
Clinical Pearls
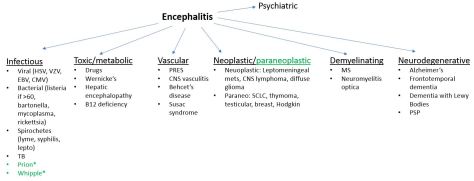
- Rapidly progressive encephalitis should trigger prion disease, paraneoplastic encephalitis, or Whipple’s!
- Most common malignancies associated with paraneoplastic encephalitis are SCLC, testicular tumors, thymomas, breast cancer, and hodgkin lymphoma
- >90% of cases of CJD are sporadic
- Definitive diagnosis of CJD is made by brain biopsy. CSF testing of 14-3-3 protein marker and the RT-QuIC protein assay combined have sensitivity and specificity >90%.
- If prion diseases are on your differential, be sure to let infection control know before doing an LP because strict precautions are required to prevent spread of infection!
Encephalitis:
Defined as AMS > 24 hours plus 2 of the following:
- Fever
- Focal neurologic deficit
- Seizure
- CSF pleocytosis
- Abnormal findings on EEG or neuroimaging
Differential
Prion diseases:
- AKA transmissible spongiform encephalopathies
- Rare, closely related, fatal, neurodegenerative conditions
- Occur in humans and mammals
- Result of accumulation of aggregated forms of the prion protein in the CNS
- >90% are sporadic, the rest are infectious (kuru, variant CJD, and iatrogenic CJD)
- Iatrogenic mostly resulting from receipt of growth hormone prepared from cadaveric pituitaries and contaminated cadaveric dura mater allografts
- Sporadic is not transmissible by blood
- Kuru was the first one recognized to be transmissible and linked to cannibalism among tribes in New Guinea
CJD:
- Most prominent clinical feature is disordered cognition
- Typically, patients also have motor signs, such as ataxia or spasticity, vague sensory problems, or changes in visual perception
- Myoclonus is common
- Progressive neurologic decline resulting in death within 6-12 months
- One in a million
- Mean age of onset 57 – 62
- More common in white people (may be ascertainment bias)
Diagnosis:
- Elevated CSF levels of 14-3-3 are not very sensitive or specific. Adding RT-QuIC protein assay to the test increases both sensitivity and specificity to >90%.
- CDC requires the following criteria for diagnosis:
- Progressive dementia AND
- 2 of the following: myoclonus, visual or cerebellar disturbance, pyramidal/extrapyramidal dysfunction, akinetic mutism AND
- Atypical EEG and/or positive 14-3-3 CSF assay with clinical duration to death <2 years and or typical MRI abnormalities (see nice example here)
Prognosis:
- Poor, majority die within 1 year
- No treatment available
