Today Elise presented a case of a middle age woman, with a history of schizoaffective disorder and recent psych med changes, who came in unresponsive and mute. She was hypertensive and catatonic on exam but afebrile. Labs revealed moderately elevated CK. She responded well to IV Ativan. The final diagnosis was drug-induced catatonia!
Catatonia
- Features:
- Hypokinesis or akinesis
- Excessive purposeless movements
- Mutism
- Decreased alertness/response to stimuli
- Negativism (resistant to all instructions, commands)
- Posturing
- Fixed stare
- Echolalia (repetition of another person’s words) or echopraxia (repetition of another’s actions)
- Subtypes
- Retarded Catatonia:
- Mainly negativism, hypokinesis, mutism, staring.
- +/- anorexia, incontinence, stupor
- Excited catatonia:
- Hyperkinesis, restlessness, impulsivity, aggression
- Malignant catatonia
- Life threatening: Fever, autonomic instability (labile BP, tachycardia, tachypnea, diaphoresis), delirium, rigidity.
- Labs: Leukocytosis, elevated CK
- Thought to be a spectrum of NMS
- Management:
- Withdrawal of offending medication if suspecting drug-related
- Initial treatment: Benzos, if pt improves with the “benzo challenge,” then this supports the dx of catatonia.
- Electro-convulsive therapy is an option.
- Retarded Catatonia:
NMS
- Tetrad:
- Encephalopathy
- Muscular rigidity (lead pipe)
- Hyperthermia
- Autonomic instability
- Associated with antipsychotics exposure, even some anti-emetics.
- Can present days to weeks after exposure.
- Management: DC offending agent, benzos, bromocriptine, supportive measures

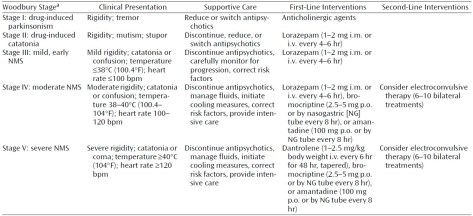
NMS can be a spectrum:
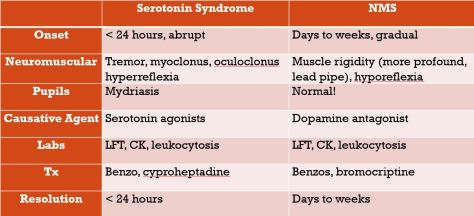
NMS can be confused with Serotonin Syndrome! Key to get a detailed medication history since SS is due to Serotonin, and NMS is due to Dopamine pathways! There are certain clues on the exam and presentation that can distinguish the two: