
Thanks to Eric for presenting the case of an “late middle-age” woman with chest pressure, found to have ST depressions, troponin elevation, TTE with apical akinesis, and clean coronaries on cardiac cath concerning for Takotsubo cardiomyopathy.
Clinical Pearls
- Think of heart failure as ischemic vs non-ischemic
- Most common causes of heart disease are ischemia (CAD), HTN, idiopathic, valvular, infectious (viral), and drugs.
- MINOCA or myocardial infarction with nonobstructive coronary arteries is MI in the absence of coronary artery disease with >50% vessel occlusion and includes the following etiologies
- Stress induced cariodmyopathy (Takotsubo)
- Coronary vasospasm
- Microvascular dysfunction
- Takotsubo cardiomyopathy most commonly presents in postmenopausal women and triggered by physical or emotional stress. The pathogenesis is not well understood and the course is self-limited. Treatment is largely supportive. Prognosis to recovery of cardiac function is 1-4 weeks.
Heart failure
- Ischemic
- CAD
- Bridge
- Non-ischemic
- HTN
- Valvular disease
- Idiopathic
- Infectious (viral is most common)
- Infiltrative (sarcoid, amyloid, hemochromatosis)
- Stress induced cardiomyopathy (Takotsubo)
- Arrhythmia
- High output (secondary to anemia, Paget’s disease, pregnancy, AV fistula, beriberi, hyperthyroidism)
- Post-partum
- Hypothyroidism
- OSA
- Connective tissue disease
MI with non-obstructive coronary arteries (MINOCA)
- Diagnosis: requires the following
- Clinical documentation of MI
- Exclusion of obstructive CAD
- No overt cause for acute MI present
- Etiologies: significant overlap with non-ischemic causes of heart failure
- Non-cardiac
- Reduced troponin clearance (i.e. renal impairment)
- Increased right heart pressures (ex PE)
- Cardiac causes
- Stress induced cardiomyopathy
- Inflammation (myocarditis)
- Coronary artery spasm (vasospastic angina)
- Microvascular dysfunction (microvascular angina, microvascular spasm, coronary slow flow phenomenon)
- Thrombophilia
- Non-cardiac
- Work up
- MINOCA is a working diagnosis
- Exclude non-cardiac cause
- Rule out ischemic etiology
- TTE
- Cardiac MRI is often indicated
- Provocative spasm testing (with acetylcholine etc in the case of coronary vasospasm)
- MINOCA is a working diagnosis
Takotsubo cardiomyopathy
- First described in Japan in 1990
- It is the underlying etiology in ~1-2% of patients presenting with ACS
- More common in post-menopausal women (mean age 66.4)
- Pathogenesis:
- Not well understood
- Clinical manifestations
- Often triggered by emotional or physical stress but ~30% of the time, no trigger is identified
- Symptoms
- Most commonly present with acute substernal chest pain. Less commonly present with SOB or syncope or heart failure symptoms
- Exam
- May have late peaking systolic murmur similar to HOCM
- EKG changes:
- ST elevation in anterior leads (43.7%)
- ST depression (7.7%)
- QT prolongation, T wave inversion, abnormal Q waves
- Troponin elevation in most patients (mean initial troponin is ~7-8)
- Diagnostic criteria
-
Transient LV systolic dysfunction (hypokinesis, akinesis, or dyskinesis), wall motion abnormalities that extend beyond a single epicardial coronary distribution
-
Absence of CAD based on cath
-
New EKG abnormalities
-
Absence of pheochromocytoma or myocarditis
-
- Work up
- Rule out ACS
- Cardiac MRI to rule out other causes of MINOCA
- Management
- Supportive
- Prognosis
- Recovery in 1 to 4 weeks
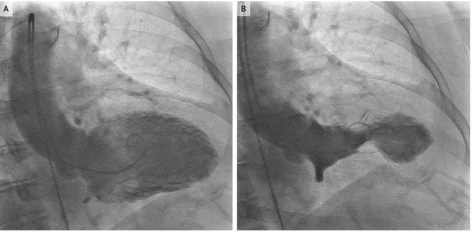
Picture above and cool video from NEJM here.
