
Today Arthur presented a case of a young woman with a personal and family history of facial swelling presenting with acute onset periorbital and scalp swelling, in setting of recent hair-dye exposure. No urticaria or pruritus on presentation but she did have acute pruritus after exposure to the hair-dye. She responded quickly to benadryl and steroids. The final diagnosis is allergic angioedema.
What is angioedema? It is a non-pitting swelling of the deep/subcutaneous tissues.

(Image adapted to JAMA)
Pathophysiology of angioedema
- Mast cell mediated (most common)
- Examples: Food allergies, insect stings
- IgE -> Mast Cells -> inflammatory response
- BeE, FoodiE = IgE
- Findings:
- Flushing
- Urticaria
- Generalized pruritus
- +/- bronchospasm, throat tightness, hypotension
- Onset: Minutes after exposure, develop over the next few hours
- Recovery: 24-48 hours
- Anaphylaxis = life threatening systemic reaction which is a severe manifestation of an allergic reaction. Angioedema is a finding.
- Management: IM Epi is FIRST LINE, 0.3 – 0.5mg IM, repeat Q5-15min PRN. Everything else (steroids, benadryl, anti-histamines) are adjuvant only. Get that IM Epi stat.
- Bradykinin mediated
- Examples: Acquired angioedema (AAE, associated with underlying malignancy or autoimmune conditions), RAAS-blocker angio edema (RAE, African Americans are 3x likely vs Whites), hereditary angioedema (HAE, autosomal dominant mode of inheritance)
- Findings:
- Absent urticaria/pruritus, bronchospasm.
- Minimal skin findings but can have swelling without urticaria.
- Onset: More prolonged course, can develop over 24-36 hours
- Recovery: 2-4 days
- Management: depends
- Histamine/Unclear: Seen in idiopathic angioedema (IAE)
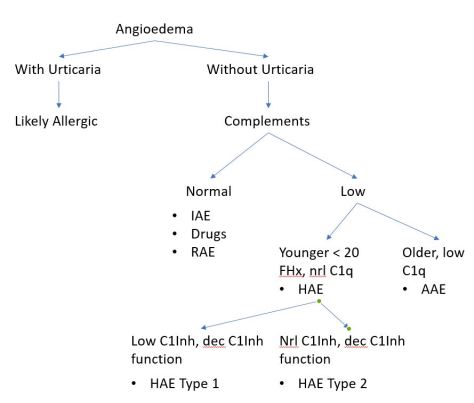
Angioedema algorithm
HAE Management
- C1 Inh concentrate (takes a while to obtain)
- Icatibant (synthetic bradykinin receptor antagonist)
- Ecallantide (recombinant plasma kallikrein inhibitor)
- FFP (fastest to get!)
- Supportive care, airway monitoring

Thank you for sharring this
LikeLike