
Yves-Paul presented a case of a middle age man with poorly controlled diabetes presenting with acute onset sore throat, which quickly progressed to dyspnea and dysphagia. He was noted to have stridor on evaluation and he was urgently intubated for airway protection. Subsequent endoscopic exam revealed a grossly purulent and inflamed epiglottis consistent with an abscess.
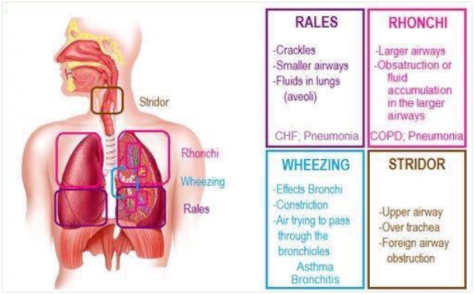
Stridor vs Wheezing
- Stridor: Upper airway, inspiration, single pitch (remember the sound quiz we did?)
- Wheezing: Relatively lower airway, expiratory musical sounds, but in bad cases can see wheezing in both
Epiglottitis
Epidemiology
- Kids more common (H. influenzae type B) but less common now due to vaccination.
Risk Factors
- Kids: Immune deficiency, incomplete immunization
- Adults: Immune deficiency, diabetes
Presentation: Drooling, dysphagia + odynophagia, dyspnea/distress
- Acute in adults over 24-48 hours Kids can be hyperacute (< 12 hours) leading to airway compromise.
- Obstruction less acute in adults due to larger AW diameter
- Sore throat and odynophagia in most cases
- Fewer have airway compromise; signs to look for are:
- Drooling
- Muffled voice
- Respiratory distress
- Stridor (impending obstruction)
- Tripoding, extended neck (maximizes airway diameter)
Diagnosis:
- Lateral X-ray with thumb sign demonstrates an enlarged epiglottis.

- Direct visualization (fiber optic), beefy red, stiff, edematous epiglottis is diagnostic.

As you can see, the surrounding structures were grossly edematous and inflamed to the point we cannot identify the vocal cords at all.
Pathophysiology
- Organisms: Strep, staph, non-type H.influenzae, beta hemolytic strep, Klebsiella
- Viral: HSV, EBV, Para/influenza, VZV
- Non-infectious: Foreign body
Management:
- Secure airway FIRST. No not manipulate or remotely touch. Can be nasotracheal or orotracheal. If unable to intubate, tracheostomy can be done.
- Abx: Beta lactamase resistant class (usually 3rd gen cephalosporin) in general unless also suspecting staph/strep, then add vancomycin as well
- I&D if abscess

