
Yonglu presented a middle age man with no medical history presenting with syncope. In the preceding months, he has been having non-specific fatigue, decreased exercise tolerance, dizziness, and diaphoresis. He was found to be hypoglycemic after this syncopal episode, and in the hospital his labs were consistent with hyperinsulinism when he was in a hypoglycemic state. CT revealed diffuse liver masses concerning for HCC, as well as a lesion on his left iliac crest appearing to be an osteosarcoma. He was also found to have a pancreatic mass as well…
Three malignant processes? Octreotide scan revealed increased uptake at these regions, and biopsy of the liver revealed a diagnosis of a neuroendocrine tumor!
Hypoglycemia
When we think about hypoglycemia, its pattern can actually give us a clue.
- Fasting: Most common
- Post-prandial: non-insulinoma pancreatogenous hypoglycemia syndrome (NIPHS), post-bariatric surgery hyperinsulinemic hypoglycemia
- Both: Insulin autoantibody, insulinoma
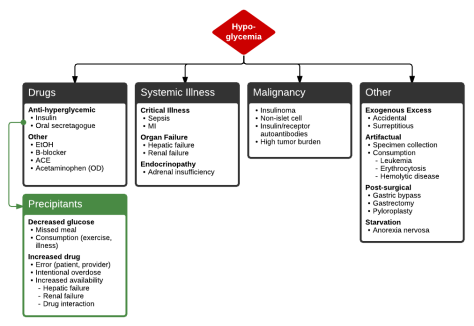
Source: grepmed
Insulinoma
Epidemiology
- Rare, not enough data
- Small cohort: median age 48 years, 77% men
- MEN Type 1: Younger presentation, 20s
Pathophysiology
- Pancreatic islet cell origin
- Generally benign, single vs multiple
- Rare to be malignant (10%)
Presentation
- Pattern: fasting hypoglycemia mainly but can be both
- May have some sympathoadrenal sx i.e. palpitations, diaphoresis (seen in this patient), tremulousness
- Likes to spread to liver, rarely can have bony mets (~13%)
Whipple’s Triad: Presence of all three demonstrates “true” hypoglycemia
- Symptoms of hypoglycemia
- Low plasma glucose at time of symptoms
- Relief of symptoms when glucose is back to normal
Diagnosis
- Evidence of inappropriately high serum insulin during episode of hypoglycemia
- 72 hour fasting plasma glucose test: Supervised fast in order to bring on hypoglycemia in order to evaluate etiology. If pt has underlying hyperinsulinism, 95-99% of the time they will be hypoglycemia within 48 hours of fasting.
- Blood test is drawn when pt has sx of hypoglycemia
- Test: Glucose, insulin, proinsulin, and c-peptide level.
- Normal: suppression of endogenous insulin
- Abnormal: Inappropriately elevated insulin, pro-insulin, and c-peptide in setting of hypoglycemia.
- Octreotide scan: Increased uptake seen in tumors of neuroendocrine etiology, more sensitive than US, CT, or MRI for detection of somatostatin receptor positive tumors
- Evidence of hyperinsulinism
- Low BHB
- High insulin level
- High C-peptide
- High pro-insulin
- Chromogranin A: used to help diagnose carcinoid tumors (NET of the digestive tract and lungs). Nowadays carcinoid is generally used to refer to well differentiated NETs originating in the lungs. GI tract tumors are now termed NET.
Management
- Localized lesion: Surgical resection is curative
- Hypoglycemia
- Somatostatin analogy
- Octreotide: Inhibits growth hormone secretion, can switch to Q-monthly formulation
- Lanreotide
- Diazoxide: Diminishes insulin secretion, side effects include hirsutism and edema
- Somatostatin analogy
- Radiation therapy: Data also limited in utility but can be consider if evidence of bony mets (which is also rare for NET)
- Chemo:
- Minority of NET, namely high-grade, well differentiated with Ki67 index > 20%, are rare and there is no consensus on how to treat these patients. These patients generally respond poorly to platinum/etoposide based regimens used to treat most NETs.
- Other options: Temozolomide, Sunitinib (RTK inhibitor), Everolimus (mTOR inhibitor)
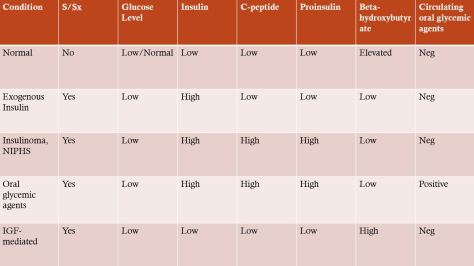
Helpful table for hypoglycemia work up.
Beta-hydroxybutyrate (BHB) is by product of alternate metabolism (more specifically ketone bodies) in a fasting state, so it can be elevated in setting of prolonged fasting (not just DKA).
Also thanks to Arathi for pointing out that insulin has a negative feedback on this process, hence in a hyperinsulinemic state (despite concurrent hypoglycemia), beta hydroxybutyrate would be very low!
Insulinomas can appear like hypoglycemia secondary to oral glycemic agents, but the key is the oral glycemic agent screen would be positive in the latter case!
IGF-omas can cause s/sx hypoglycemia due to similarity with insulin. Expect IGF2 levels to be elevated in such cases and elevated BHB.
Please refer to this helpful review article if you want to know more about NETs!
Also please refer to this paper for a case report on AFP-producing pancreatic NET (AFP elevated in this patient!)
