
Our doctor-in-training, Jacqueline, presented a case of a 46yo man with a complicated abdominal surgical history, as well as schizophrenia, who presents with acute onset vague abdominal pain. He could not provide any remarkable history (other than abd pain and losing a bag of coins), and his exam was otherwise benign except for mild diffused abdominal pain…
The mystery was resolved on a radiography.
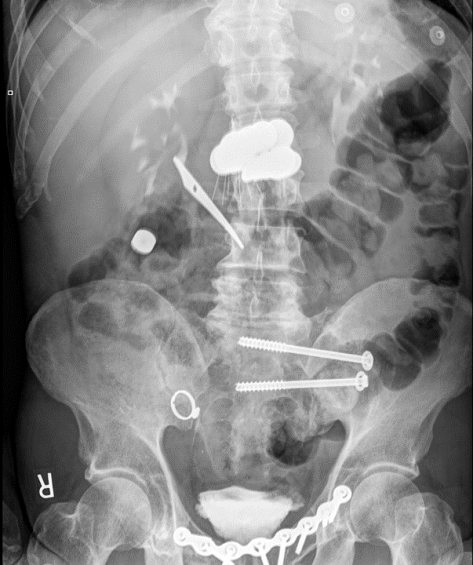
Foreign Body Ingestion
Epidemiology
- Mostly in kids, peaks 1-2 years of age
- Adults: Typically, accidental (95% of cases) usually related to fish, chicken bones, or toothpicks. More common in older adults, pts with mental illnesses, intoxicated, or inmates (drug trafficking, packers vs stuffers).
- Most frequent cause of esophageal obstruction = food bolus on existing stricture
Presentation
- Asymptomatic
- Stridor/airway compromise/aspiration
- Chest pain/abdominal pain
- Fever, shock (perforation)
- Hemoptysis, hematemesis
Diagnosis
- Imaging, clinical history
Management:
- Will depend on stability, the location, nature of the objects ingested, and progression.
- Expectant management for most blunt objects, ~ 70-80% of objects will pass by day 4. Consider surgical/endoscopic intervention if failure to progress
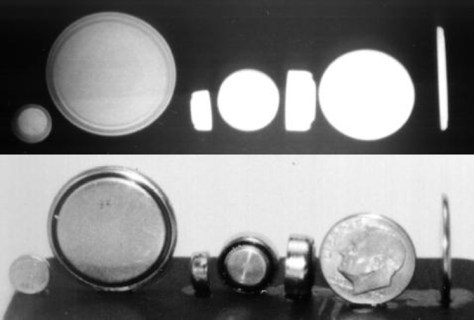
Battery
- Presentation
- Local necrosis secondary to pressure, electrical current, or caustic chemicals.
- Ulceration can occur within 2-4 hours
- Perforation can be seen as early as 4-8 hours
- VERY IMPORTANT to distinguish between coin batteries (thicker, concentric circles) vs coins (thinner, confluent)!
- Complications
- Vocal cord paralysis, esophageal perf, stricture, tracheal/esophageal fistula, aspiration pneumonia, mediastinitis, erosions into arteries, gastric hemorrhage, intestinal perf
- Management
- Esophagus: Emergent removal
- Beyond esophagus: Depends, most (89%) will pass within 7 days
- Surgical/Endoscopic option: consider if co-ingestion of magnets, or if remained in stomach for more than 48 hours.
- GI symptoms
- Cylindrical batteries: Relatively harmless and usually pass through GI tract without issues, but if stuck in stomach or esophagus, endoscopic removal is recommended
Magnets
- Presentation
- Fistula, perforation, volvulus, obstruction, localized necrosis (pressure)
- Higher chance of complications if multiple magnets and/or metallic objects were ingested.
- Can react with metal external of the body and cause injury
- Complications
- Localized bowel necrosis, obstruction
- Management
- Prompt removal endoscopically if in esophagus or stomach.
- Beyond stomach: Surgery if symptomatic or failure to progress
- Single magnet: Expectant management, serial XR, monitor progress, don’t be around anything ferromagnetic
Sharp
- Presentation
- High risk of perforation/injury if in esophagus, medical emergency
- Complications
- Esophageal perforation
- Intestinal perforation
- Management
- Immediately endoscopic removal if in esophagus
- Beyond:
- Stomach/proximal duodenum: still consider urgent endoscopic removal, complication risk varies from as low as 10% to 40%
- Beyond and failure to progress: Surgical intervention recommended.
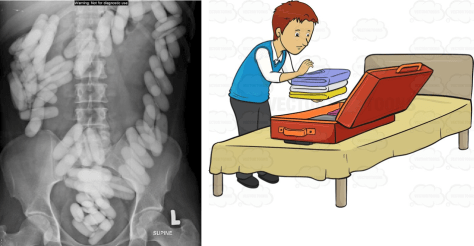
Packers vs Stuffers
- Packers: Carefully PACKING illicit substances into packages, lower chance of leakage (image adapted from Vectortoons.com)
- Stuffers: Hastily STUFFING illicit substances to hide evidence from law enforcement (image adapted from Family Guy), higher chance of content leakage.
- Management:
- Decontamination:
- Packers: Whole-bowel irrigation safe and feasible
- Stuffers: Controversial
- Symptomatic:
- Opioid (CNS depression, hypoventilation, pinpoint pupils): IV Naloxone 0.05 in nonapneic patients, 0.2 – 1mg in apneic patients. Larger doses may be required if pt ingested a large amount of heroin.
- Sympathomimetic (agitation, hypertension, hyperthermia): Symptomatic management, airway monitoring, temperature control. AVOID pure beta blockers. Can consider GI decontamination but consult Poison Control.
- Decontamination:

If suspecting ingestion of potentially toxic substance, don’t hesitate to call Poison Control!

