The world’s #1 addictive substance of choice… Caffeine! And yes you can OD on it!
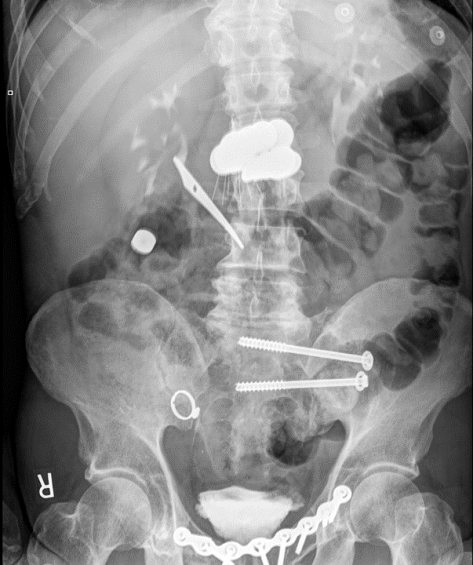
A 37yo F with history of anxiety presented with nausea and palpitations after ingesting 160 pills of Diurex in an attempt to fix her constipation for the past 2 weeks. Prior to arrival to the hospital, the paramedics administered activated charcoal. She was tachycardic, mildly hypotensive, hypokalemic, and acidotic (AG 20). Methamphetamine was found in her system as well. Fortunately she improved with fluids and supportive measures, but lethal cases of caffeine overdose, while rare, have been described in the medical literature!
Of note: An expresso doubt shot contains roughly 60-100mg of caffeine.
This patient took 16000mg (16g) of caffeine, equivalent to 160-260 shots of double expresso!
Caffeine Intoxication
- Epidemiology
- Caffeine = world’s #1 psychoactive compound consumed
- Pure caffeine can be easily obtained, caffeine pills introduced in 2004.
- Death from caffeine overdose is rare, only 92 cases have been described in literature.
- Caffeine pills heavily advertised as weight loss supplements
- Risk factors
- Psychiatric conditions
- Athletes (weight loss/work out supplements, these things are NOT regulated!)
- Infants/young kids (accidental ingestion)
- Pathophysiology
- Dose-dependent MOA
- CNS and cardiac stimulation, usually occurs at plasma concentration of 15mg/L or higher
- Usually not food/beverages related. Most cases are related to caffeine-containing medications.
- Lethal cases reported over 10g ingestion, highest reported ingestion is 100g (1000 double shots of Expresso)
- Absorbed in the GI tract within 30 minutes
- Half life 5-6 hours, metabolized in the liver
- Presentation
- Agitation, diaphoresis, anxiety, restlessness, insomnia, GI disturbances, tremors, psychomotor agitation
- Complications
- Serious cases: arrhythmias (SVT, VT), even V-fib (most common cause of death in caffeine intoxication)
- Hypotension
- Hypokalemia
- Seizures
- Lactic acidosis
- Rhabdomyolysis
- Renal failure
- Diagnosis
- Life threatening caffeine overdose more commonly associated with blood concentration > 80mg/L
- Clinical history, serum measurement, ingestion history
- Management
- Activated charcoal for ingestions:
- Effective only within a short time of ingestion, typically within 1-2 hour and patients have to be mentating
- Interacts with caffeine and prevents it from being absorbed.
- Hydration
- Electrolyte repletion
- Anti-arrhythmic agents (amiodarone, even lidocaine) in setting of arrhythmias, ACLS if unstable arrhythmias
- Dialysis: Dialyzable
- Activated charcoal for ingestions:
Source: Grepmed
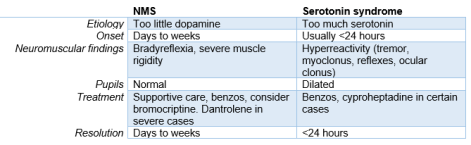
A summary of toxidromes: