Today, we discussed the case of an elderly woman with significant history of vasculopathy and ESRD who presented with weakness, found to be bradycardic to 30s, hypotensive, and hyperkalemic to 7.2. Her hyperkalemia was treated with dialysis but she underwent cardiac cath due to up trending troponins, found to have a 100% occlusion of the RCA!
Clinical Pearls
- First step in managing a patient with bradycardia is ABCs!
- First medication for symptomatic bradycardia is atropine. Remember that atropine works at the level of the AV node and higher so if the block is occurring somewhere below the AV node, then atropine will not be effective.
- Other pharmaceutical agents are dopamine, epi, or isoproterenol
- Anyone with bradycardia and unstable hemodynamics in spite of above treatments should receive transcutaneous pacing. This buys you time until you can place a transvenous pacemaker (less painful, more effective)
- ECG has a low sensitivity but high specificity for hyperkalemia-induced cardiomyocyte instability.
- ECG changes associated with hyperkalemia in progressive severity:
- Peaked T waves
- P wave widening, PR prolongation, P wave disappearance
- QRS widening, AV block, bradycardia
- Sine wave
- VF/asystole/PEA
Bradycardia approach
1. ABCs!
- Pharmaceutical agents
- Atropine (0.5 mg – 1 mg q3-5 mins for a total of 0.03 mg/kg)
- If no improvement, consider dopamine or epi
- If still symptomatic, then start transcutaneous pacing
2. Find underlying cause and treat it
- Meds: BB, CCB, amio, digoxin, clonidine, lithium, acetylcholinesterase inhibitors
- Ischemia (up to 25% of patient with acute MI present with bradycardia)
- ↑ vagal tone: if young, athlete
- Metabolic: hypoxia, sepsis, ↓T4, hypothermia, hypoglycemia, hyperkalemia
- OSA
- Elevated ICP
- Infections: legionella, lyme, Q fever, typhoid, malaria, RMSF, yellow fever, leptospirosis, dengue, Chagas disease
- Infiltrative processes: sarcoid, amyloid, hemochromatosis
In our patient, the cause was severe hyperkalemia as well as an RCA infarct. Given her clinical instability, and the potential for worsening hyperkalemia from cardiac catheterization alone, the team normalized her serum potassium before performing cardiac cath which led to the RCA MI diagnosis.
Hyperkalemia
- ECG changes are not sensitive for hyperkalemia and can miss up to 39% of patients even with a K of 7-9.
- Sweet spot for potassium appears to be a mean K of 3.5 to 4.5 mEq/L. There is not a well-defined treatment threshold.
- Bottom line for management: if you have the kidneys available, use the kidneys to excrete as much potassium as possible.
- Newer agents like sodium zirconium and patiromer. Mix with water. Well tolerated and highly effective.
Agents that reduce serum potassium via transient intracellular shift:
- Insulin: give with D50 if normoglycemic to avoid hypoglycemia and be sure to check FSG hourly for 4 hours after to ensure no hypoglycemia develops
- Albuterol (10-20 mg) nebs: this is significantly higher than the dose we give in COPD (2.5 mg) and is equal to ~8 treatments! So make sure to continue the nebs when the patient arrives on the floor from the ER if they are still hyperkalemic.
- NaHCO3: best for management of chronic hyperkalemia in the outpatient setting. In the acute management of hyperkalemia, alkalinization of serum with a large bicarb load can lead to a reduction in serum calcium levels. Lower serum calcium can lead to more cardiac membrane instability and fatal arrhythmias!
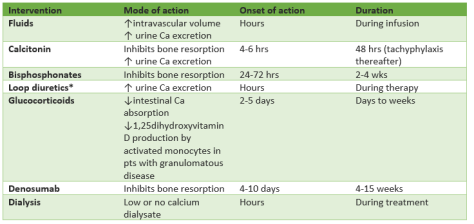
Agents that eliminate potassium from the body:
- Loop diuretics: first choice if a functioning kidney is available!
- Cation exchange binders: preferred when kidneys are not available
- Patiramer (available at VMC), much more tolerable than kayexalate and highly effective at lowering serum potassium. Like kayexalate, it works over hours to days.
- Sodium zirconium: similar to patiramer but not currently available
- Kayexalate: not pleasant to take orally. Also carries with it the slight risk of colonic ischemia especially in post renal transplant patients and those with baseline colonic dysfunction (due to infection or inflammation).
- Dialysis
Indication for using calcium gluconate: when EKG changes are noted. Repeat doses (maximum 3) until EKG changes have resolved.
EKG Changes in Hyperkalemia:
- K > 5.5 ⇒ repolarization abnormalities:
- Peaked T waves are the earliest sign
- K > 6.5 ⇒ progressive paralysis of the atria:
- P wave widens and flattens
- PR segment lengthens
- P wave eventually disappears
- K > 7.0 ⇒ conduction abnormalities and bradycardia:
- QRS widens
- High-grade AV block, slow junctional and ventricular escape rhythms
- Any kind of conduction block (bundle branch blocks, fascicular blocks)
- Sinus bradycardia or slow AF
- Sine waves
- K > 9.0 ⇒ cardiac arrest:
- Asystole
- Ventricular fibrillation
- PEA with bizarre, wide complex rhythm