Thanks to Erica for presenting the case of a middle aged man who presented with acute back pain and B symptoms after trauma to his back, found to have stage 3B multiple myeloma.
Clinical Pearls
- Remember that majority of cases of acute low back pain (<6 weeks) is due to musculoskeletal etiologies that spontaneously improve on their own. Imaging and further diagnostic work up is not indicated unless there are red flags (see below).
- A straight leg test is more useful when negative as it has a high negative predictive value for ruling out radiculopathy. False positive rates are quite high.
- Unexplained anemia and worsening renal function in the outpatient setting should trigger a work up for multiple myeloma.
- The most common presenting symptoms for MM are anemia (73%), bone pain (58%), and renal insufficiency (48%).
- In diagnosing MM, sensitivity increases with each added test: SPEP (82%) → IFE (93%) → FLC/UPEP (97%). The other 3% that would not be diagnosed with these tests have a non-secretory MM (monoclonal increase in plasma cells in bone marrow that do not produce immunoglobulins or light chains).
Red flags for acute low back pain:
- Focal neurologic complaints/deficits
- History of cancer
- Age >50 years
- Fever not explained by another cause
- History of recent bacteremia or IVDU
- Steroid use
- Weight loss
- Pain that is worse at night
- No relief with bed rest or pain lasting >1 month
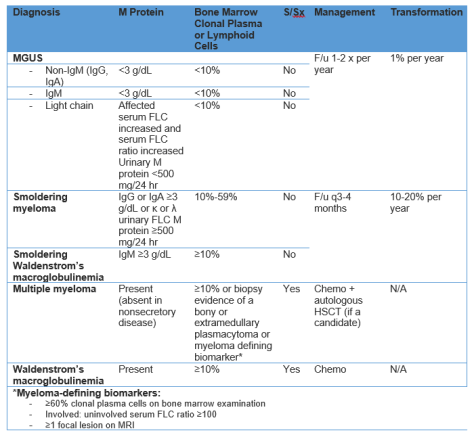
Multiple Myeloma: refer to this prior blog post. Other info below:
Diagnostics:
- SPEP: picks up M protein or elevated immunoglobulins (heavy + light chain) in the serum. You can diagnose over 80% of patients with MM using an SPEP.
- IFE: identifies the specific type of immunoglobulin that is elevated with its light chain.
- Free light chains (FLC): measures the amount of free light chains not bound to a heavy chain floating around in the blood. Normally people have about a 2:1 ratio of kappa to lambda chains. In light chain only multiple myeloma, there is a disproportionate increase in one type over the other and the ratio will be off. If there is an increase in both light chains but the ratio is normal, think kidney disease!
- Keep in mind that the reason to check FLC when you suspect MM is to diagnose those people who are only producing light chains and not whole immunoglobulins that would have been picked up by SPEP/IFE.
- UPEP: measures light chains dumped in the urine (Bence Jones protein)