
Thanks to John for presenting the case of a middle-aged woman with metastatic renal cell carcinoma who presented with subacute diffuse weakness and constipation, found to have symptomatic hypercalcemia, treated with IV fluids and zoledronic acid.
Clinical Pearls
- A third of patients with malignancy develop hypercalcemia in their disease course. Hypercalcemia of malignancy is associated with very poor prognosis (~50% 30 day mortality).
- Constipation plus polyuria is the most specific symptom combination for hypercalcemia
- Denosumab is superior to zoledronic acid in treating hypercalcemia of malignancy and is safe to use in renal failure.
- One way to quickly determine the etiology of hypercalcemia from your chemistry panel is to look at the chloride to phosphate ratio. A ratio > 33 is highly suggestive of a PTH or PTHrP mediated process.
Hypercalcemia ddx:

** Primary hyperPTH is the most common cause of hypercalcemia in the outpatient setting. Malignancy is the most common cause of hypercalcemia in the inpatient setting.
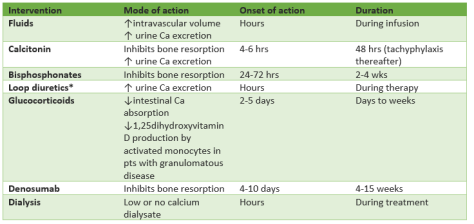
Treatment of hypercalcemia:
Ca <12
- No treatment if asymptomatic
- Avoid exacerbating factors
Ca 12-14
- If chronic/asymptomatic ⇒ same tx as Ca <12
- If acute/symptomatic ⇒ same tx as Ca 14-18
Ca 14-18
- IVF – lots!
- Lasix only if concurrent renal/heart failure
- Calcitonin
- Bisphosphonate (zoledronic acid >>pamidronate if malignancy. Denosumab if refractory to ZA or severe renal impairment)
Ca >18
- Above PLUS
- Hemodialysis

One thought on “Hypercalcemia of malignancy”