
Today we discussed an interesting case of acute encephalopathy due to hypercalcemia of malignancy due to bone metastases.
We first reviewed the importance of maintaining a broad differential for acute encephalopathy/delirium/acute confusional state/AMS.
We reviewed the following framework:
Neurologic / Toxic / Metabolic / Infectious / Other.
We then reviewed the differential for hypercalcemia. For those of you interested, please check out this awesome review video by Dr. Strong:
Our patient had hypercalcemia of malignancy and the following patients were made:
- It is the most common cause of hypercalcemia in inpatients
- The most commonly associated malignancies are breast, lung, multiple myeloma, and renal
- There are three major mechanisms for hypercalcemia of malignancy
- Secretion of PTHrP – 80% of malignancy related hyperCa
- Osteolytic Metastases – ~20% of cases
- Increased 1,25-OH-Vitamin D (calcitriol) 2/2 to increased 1-alpha-hydroxylase activity from activated macrophages in lymphomatous (and also granulomatous) tissue
- We reviewed the PTH-based algorithm and determined that it was a PTH-independent process (PTH low or low-normal) and then used the PTHrP, calcidiol and calcitriol to guide to the correct diagnosis which was confirmed by MRI and bone scan
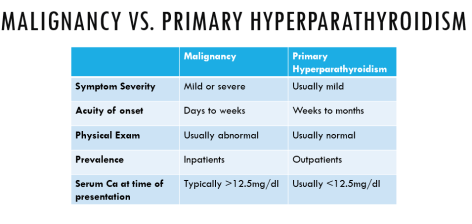
Finally, here is a way to distinguish between malignancy related hypercalcemia and primary hyperparathyroidism (most common cause in outpatients & higher co-occurrence in patients with malignancy)
For treatment options, please see the following blog post for more details!
