Today we talked about the case of a young woman who presented after suicide attempt by ingestion of multiple prescription medications, found to be obtunded, initially in status epilepticus and later with exam findings concerning for serotonin syndrome.
Clinical Pearls
- Continuous EEG is indicated if a patient is not returning to baseline mentation 15 mins after a seizure to rule out non-convulsive status epilepticus.
- Status epilepticus is defined as a seizure lasting > 5 mins or > 2 discrete seizures between which there is incomplete recovery of consciousness.
- Treatment of status epilepticus involves acute management with IV/IM benzos, urgent long-term control with IV fosphenytoin (preferred), phenytoin, or valproic acid. Remember that keppra is more useful in suppressing future seizures than treating an acute episode.
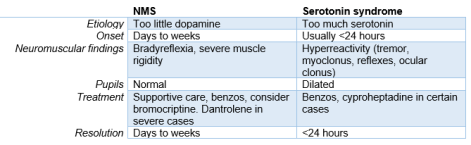
- Serotonin syndrome is a clinical diagnosis and manifests with neuromuscular activation like tremors, hyperreflexia, and clonus (generally worse in lower extremities). Use Hunter’s criteria to help with diagnosis.
Status Epilepticus
- When is continuous EEG needed?
- If patient is not returning toward baseline in 15 mins after a seizure, goal is to rule out nonconvulsive seizures
- How to define status?
- > 5 mins OR
- > 2 discrete seizures between which there is incomplete recovery of consciousness
- Non-convulsive status epilepticus
- Suspect if LOC not improving by 10 mins after cessation of movement
- Mental status remains abnormal for 30-60 mins after movement cessation
- Dx requires a 24-hour EEG (we don’t have one ☹)
- Treatment is the same as generalized status epilepticus, but prognosis is worse (mortality 65% vs 27%)
- Treatment of status
- Assessment and supportive treatment
- Initial pharmacologic therapy
- Ativan (2 mg IV q1-2 mins), total dose 0.1mg/kg
- Watch out for respiratory depression and hypotension
- Alternatives: versed 0.2mg/kg IM, valium 0.2mg/kg IV
- Ativan (2 mg IV q1-2 mins), total dose 0.1mg/kg
- Urgent long-term control
- Fosphenytoin (preferred): 20 mg/kg at 150mg/min
- Give extra 10 mg/kg if not responding
- Dephosphorylates into phenytoin. It’s more soluble in water and less likely to precipitate in the skin and vessels.
- Phenytoin: 20mg/kg at 50mg/min (slower than fospheny)
- If infused too fast, can irritate skin/vessels causing skin necrosis
- Valproic acid: 20mg/kg at 5 mg/kg/min
- Sometimes the preferred choice in patients with known generalized epilepsy b/c phenytoin can provoke absence seizures in that population.
- What about Keppra?
- Technically not FDA approved for status. It has weak evidence to support its use. More useful in suppressing subsequent seizures after status has been controlled.
- Fosphenytoin (preferred): 20 mg/kg at 150mg/min
Serotonin syndrome:
- Clinical diagnosis. Serum serotonin concentrations do not correlate with clinical findings.
- Severe disease can lead to DIC, rhabdo, renal failure, and ARDS.
- Diagnostic criteria: use Hunter’s (84% sensitive, 97% specific)

- DDx
- NMS
- Anticholinergic toxicity
- Malignant hyperthermia
- Sympathomimetic intoxication
- Sedative-hypnotic withdrawal
- Meningitis
- Encephalitis
- Serotonin syndrome may be distinguished from other causes of agitated delirium on the basis of neuromuscular findings. Whereas patients with serotonin syndrome show signs of neuromuscular activation (eg, tremor, hyperreflexia and clonus that are greater in the lower extremities, ocular clonus, and increased muscle tone), patients with sympathomimetic toxicity or infections of the central nervous system lack these findings.
- Treatment
- Supportive care and sedation
- Chemical sedation preferred over physical restraint
- Autonomic instability
- High BP: esmolol or nitroprusside (Short acting). Avoid longer acting agents
- Low BP: neo or epi. Avoid idirect agents like dopamine because they are converted to epi and norepi. When monoamine oxidase is inhibited, epi and norepi production at the cellular level is not controlled and could lead to an exaggerated HD response.
- Hyperthermia
- No benefit to Tylenol b/c increase in body temp is due to increased muscular activity rather than alteration in the hypothalamic temperature setpoint.
- If temp >41.1, then sedate, paralyze, intubate
- Antidote: cyproheptadine
- Histamine receptor antagonist. Also has weak anticholinergic activity
- 12 mg loading dose, then 2 mg q2h until clinical response is seen.
- Is sedating (good) and can also cause transient hypotension.
- Supportive care and sedation