
Narges presented a case today with a middle age woman with uncontrolled insulin dependent diabetes Type 2, multiple malignancies s/p resection, presenting with acute anasarca and shortness of breath developed over a few days. She was anasarcic up to the mid back on presentation, with an albumin of 0.9 (baseline of 3.8 a month ago). Her UA had 3+ protein and a urine protein/Cr ratio of 23. If you’re thinking nephrotic syndrome, that’s right! Biopsy revealed the diagnosis of minimal change disease (MCD) with concurrent ATN!
Nephrotic Syndrome
Some definitions
- Nephrotic range proteinuria: > 3.5g proteinuria per day or spot urine protein/cr ratio of > 3.5
- Nephrotic syndrome: Above + symptoms (edema, HLD, hypoalbuminemia, lipiduria, etc)
Epidemiology
- Most common primary cause of nephrotic syndrome in adults in the US is FSGS
- Most common secondary cause of nephrotic syndrome in adults in the US is Diabetic Nephropathy
Presentation
- AKI (underlying glomerulonephritis vs hypovolemia vs sepsis vs ATN)
- Hypercoagulability (loss of anticoagulant proteins namely antithrombin III, C, S)
- Hyperlipidemia (reactive hepatic synthesis of proteins due to hypoproteinuria)
- Malnutrition (gut edema, dec body weight, edema) leading to anemia, osteomalacia, vitamin D deficiency
- Immunocompromise (inc risk for infection due to hypoimmunogammopathy)
- Edema (low oncotic pressure due to hypoalbuminemia)
Diagnosis
- 24 urine protein > 3.5g is diagnostic
- Spot urine protein/cr ratio > 3.5 is also diagnostic
- Exactly cause will require additional work up, to be discussed below in differential
General Management Strategies
- Proteinuria control (ACEi, ARB)
- BP Control
- Volume Control (Diuretics, low salt)
- HLD: usually resolves with disease control, can use statins
- Immunosuppresion for primary causes
- Treat underlying secondary causes
Differential Diagnosis
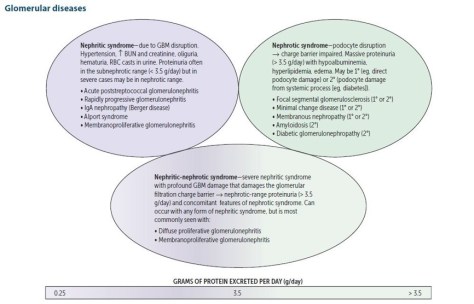
Source: Grepmed
The three most commonly encountered causes, besides diabetic nephropathy, are:

Minimal Change Disease
As seen in this patient, is typically seen in pediatric population and it is the most common cause of nephrotic syndrome in kids < 8-10 years old. It only accounts for 10% of cases of nephrotic syndrome in adults.
Presentation
- Acute onset edema
- Higher incidences of thrombotic events in adults
- AKI common, at higher risk for ATN
Diagnosis
- Biopsy, electron microscopy with podocyte effacement
Management
- Corticosteroids: initial course of 6-8 weeks in adults, 1.5mg/kg/day
- Cyclosporine for non-responders
- Other options: mycophenolate (Cellcept), azathioprine (but pt is already on this, Imuran!)
Prognosis
- 80-90% of patients respond to initial corticosteroid therapy
- Up to 50% can recur
Focal Segmental Glomerulosclerosis (FSGS)
Epidemiology
- Higher incidence among African Americans (5 times more likely than White)
- Associated with HIV (collapsing variant), heroin (30x risk)
Diagnosis
- Biopsy: focal and segmental hyalinization of the glomeruli, often with immunostaining showing IgM and complement (C3) deposits in a nodular and coarse granular patter
Management
- Primary: Immunosuppression, corticosteroids +/- cyclosporine, tacrolimus + plasma exchange
- Secondary: Treat underlying cause
Prognosis: Poor
- > 50% develop renal failure within 10 years of diagnosis, and 20% develop ESRD within 2 years despite treatment
- May recur after kidney transplantation.
- Heroin addicts with FSGS: can experience complete remission if they STOP EARLY.
Membranous Nephropathy
Epidemiology
- Associated with malignancy i.e. lymphoma, colon cancer, lung cancer
- Most cases are idiopathic
Diagnosis
- Biopsy
- Microscopy: Thickened capillary loops
- Immunoassay: Granular IgG & C3 depositions in the subepithelial layer
Management
- Immunosuppression similar to above, treat any secondary causes
Prognosis
- Generally pretty god, 30-40% treated go into complete remission, 30-50% go into partial remission. Treatment can be prolonged.
- Treating secondary causes also can induce remission.
Note that there are some other causes that can present with both nephrotic and nephritc features, i.e. membranoproliferative glomerulonephritis. Complement levels are NORMAL in MCD, FSGS, and MN, while complement levels are low in MPGN.
Primary anticoagulation for patients with nephrotic syndrome can be considered in some cases but not routinely done. Please refer to this article for reference.
