
Katie presented a case of an elderly man with history of non-anuric ESRD on HD three times a week, NIDDM2, CMML, Klinefelter Syndrome, HTN, chronic anemia, and prior GIB secondary to gastric AVM who presented with shortness of breath. Earlier during the day he was at the transfusion center where he received a unit of PRBC. He was restless after the transfusion but he refused to stay for post-transfusion monitoring. He has been compliant with dietary restrictions and his HD sessions, but that evening after he went home, he started having difficulty breathing and hence he came to the ED. He was significantly hypertensive on presentation, and he went into respiratory failure requiring NIPPV. CXR revealed significant bibasilar pulmonary infiltrates c/w pulmonary edema. After diuresis and dialysis, his symptoms resolved. This presentation is consistent with transfusion associated circulatory overload, or TACO!
Let’s use this case to go over different types of transfusion reaction since you:
- Will encounter this during your career
- Will definitely get paged about this on nights
- Might encounter the more rare but potentially life-threatening reactions
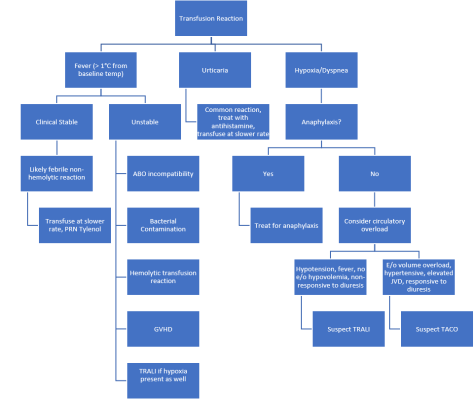
Transfusion Reaction
- Common presentation
- Fever (defined as > 1 degree Celsius from baseline)
- Stable: Likely febrile non-hemolytic transfusion reaction
- Tylenol, slow rate of infusion, observe
- Unstable
- ABO incompatibility
- Bacterial contamination
- Hemolytic transfusion reaction
- TA Graft vs Host Disease (4-30 days after, delayed rxn, attack by immunocompetent donor lymphocytes on an immunocompromised recipient’s antigen presenting tissues. In immunocompetent recipients, reaction can occur if recipient is heterozygous for an HLA for which the donor is homozygous)
- Urticaria:
- Mild allergic reaction to plasma protein, common, resume transfusion at slower rate, anti-histamine PRN.
- Dyspnea or hypoxia
- Assess for anaphylaxis
- Yes: Treat for anaphylactic allergic reaction
- No: Consider circulatory overload
- E/O vol overload, diuretic responsive: TACO (transfusion related circulatory overload)
- Signs of instability, diuretic non-responsive: Suspect TRALI
- Hemolysis 1-4 weeks after transfusion: Delayed hemolytic transfusion reaction, usually very mild
- Assess for anaphylaxis
- Stable: Likely febrile non-hemolytic transfusion reaction
- Fever (defined as > 1 degree Celsius from baseline)
TACO
Epidemiology: 1% of transfusions in general, higher in the ICU.
Pathophysiology: Circulatory overload leading to pulmonary edema
Risk Factors
- Preexisting renal or cardiac dysfunction
- Higher transfusion volume
- Small stature
- Low body weight
- Extremes of age
- Female
- White
- Hypoalbuminemia
Presentation
- Development of respiratory distress or hypertension during or within 6 hours of completing a transfusion.
- May see concurrent headache
- Hypoxia, HTN, tachycardia, wide-pulse pressure, JVD, S3, crackles/wheezing
Diagnosis
- Clinical
- Nt-proBNP elevated but non-specific
Management
- Stop transfusion
- Oxygen
- Diuresis
- Report to transfusion service or blood bank. Get consultation for future transfusions i.e. smaller units, lower volume, or only during dialysis
TRALI
Epidemiology
- Rare, estimated 1 in 12000, leading cause of transfusion related mortality in the US
- Seen in all age groups and both sexes
Pathophysiology
- Not completely understood, but thought to be a neutrophil mediated reaction in setting pre-existing endothelial injury in the lungs, or antibodies to HLA
Risk Factors
- ICU patients
- Multiparous female donors (OR 4.5)
- Heme malignancies
- Chronic EtOH
- Liver dysfunction
- Tobacco use
- Positive fluid balance
- Mechanical ventilation
- Note: Transfusion of older blood products was once thought to be a risk factor, but disproved by multiple RCTs around 2010-2012.
Presentation
- During or within 6 hours after blood product transfusion
- Hypoxia, pulmonary infiltrates on exam, fever, hypotension
- May see elevated peak/plateau airway pressures in vented patients
- Non-responsive to diuretics
- ARDS like picture, sometimes diagnosis can be unclear, recent nomenclature of transfused ARDS.
- May have coexisting TACO
Diagnosis
- Clinical
Management
- Stop transfusion
- Notify blood bank/transfusion service
- Oxygen/ventilatory support, ARDS protocol (lower tidal volume) has generally been used
- Hemodynamic support, pts often hypovolemic, give fluids, pressors if needed.
- Corticosteroid historically has been used with inconsistent results
Prognosis
- Mortality as high as 41-67% in ICU population. Non-ICU patients have much lower morality, 5-17%. Almost all will recover their resp function, and they can still safely receive blood transfusions in the future.
Prevention
- Identify implicated donor
- Irradiate blood products for immunocompromised recipients
- Avoid transfusion of blood product from a relative
- Blood donated by men has lower incidence for unclear reasons

