
Tim presented a young man with no medical history presenting with a chronic cough with intermittent trace hemoptsis. Other than this cough and mild shortness of breath when he exerted himself, this pt had no other symptoms. A CXR revealed bilateral pleural effusion, and upon thoracentesis, milky fluid drained out with an elevated triglyceride content consistent with a chylothorax. Subsequent biopsy of a lymph node revealed a diagnosis of follicular lymphoma!
Since we are talking about pleural effusion, Light’s Criteria will inevitably come up. For both real life (and boards!) purposes, know this criteria really well!
Light Criteria:
- SENSITIVE but NOT SPECIFIC for exudative effusions.

Any one of these criteria = exudative
- Fluid protein/Serum protein > 0.5
- Fluid LDH/Serum LDH > 0.6
- Fluid LDH > 2/3 upper limit of normal of serum LDH
False positive is possible in certain settings:
- Chronic diuretic use can falsely elevate fluid LDH (KNOW THIS)
- Transudative effusion that’s been sitting there chronically can appear exudative like
The following tests can help us distinguish between a falsely positive exudative effusion from a true exudative effusion:
- Pleural cholesterol > 45 mg/dL has high sensitivity and specificity for exudative effusions.
- Can also use serum albumin – fluid albumin < 1.2g/dL to confirm exudative effusion
Pleural Fluid Analysis: Clues
Upon performing a thoracentesis, certain characteristics can potentially give us some clues to the etiology of the effusion…
Fluid Color

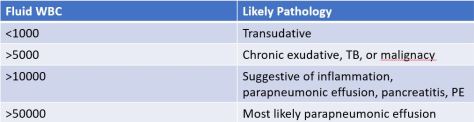
Fluid WBC Count
Fluid Predominant Myelocyte Type

Lastly, how do you diagnose a chylothorax and what are some potential causes?
Chylothorax
- Definition: Triglyceride > 110 mg/dL = slam dunk
- 50 – 110: Less clear, cannot rule out, obtain liproprotein analysis. If presence of chylomicron is detected, likely chylothorax
- < 50: Less likely
- Non-traumatic
- Malignant: Lymphomatous is most common, can also be other cancers i.e. lung, mediastinal mets, sarcoma, leukemia
- Non-malignant: Idiopathic, benign tumors, protein losing enteropathy, thoracic aortic aneurysm, TB, Sarcoid, amyloidosis, thyroid goiter, tuberous sclerosis, congestive heart failure, mitral stenosis
- Traumatic
- Surgical is most common
- External trauma
- Trivial “trauma:” Stretching while yawning, coughing, hiccupping, sneezing (I’m not kidding)
Management of a malignant pleural effusion, as seen in this case, can be potentially challenging. After the patient was discharged, his pleural effusion on the right recurred within 3 days and completely filled up his right lung!
Several options are available for management of malignant pleural effusions. The decision is complicated and will goals of care discussion
- Indwelling pleural catheter
- Advantage: Pt managed, can drain at home
- Disadvantage: Catheter related complications
- Pleurodesis
- Talc, slurry or poudrage, is the preferred agent. 60-90% success rate in reducing recurrence at 30 days.
- Doxycycline can also be used but not as popular any more
- Advantage: Eliminates the potential space for fluid reaccumulation
- Disadvantage: Pain, potential for surgical failure, invasive
- Combination: Talc + IPC
- Pleurectomy
