
Today we discussed a case of a patient who had been reporting 6 months of “dizziness”. We first took a deep dive into dizziness and what exactly it means.
The single most important question to ask a patient with dizziness is: what do you mean by that?
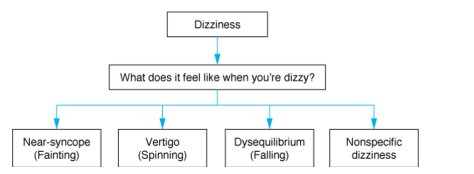
Dizziness can then be classified into four major categories depending on the description of the symptoms (though of course this slightly antiquated framework does have limitations). We emphasized the importance of not coaching the patient to using certain descriptors and also recognized the cultural differences in the usage of the term dizziness (many communities utilize this word to indicate sickness, rather than how we define it).
We focused our discussion on Vertigo as the patient reported a room-spinning sensation for the past 6 months. The major discussion is always central vs. peripheral vertigo and please see the excellent prior blog post discussing this in detail:
We reviewed some important distinguishing characteristics (as taken from a 2014 NEJM Review Article on BPPV)

The key takeaways are as follows:
1. BPPV is characterized by positional, brief (<1 minute) attacks of severe vertigo prompted by head movements and if nystagmus is seen, it is unidrectional. The typical discussion therefore is not BPPV vs a posterior CVA but rather an acute vestibular syndrome (vestibular neuritis/labrynthitis) vs. a posterior CVA.
2. If the Dix-Hallpike induces vertigo, this does not mean the patient has BPPV! The characteristics of the nystagmus however may be very helpful

3. The HiNTs exam can be exceptionally useful, but only in the right clinical context (it can only be used if the patient is currently symptomatic, and is meant for continuous, not intermittent, symptoms. (i.e hours – days)
- https://www.nuemblog.com/blog/hints
- Recognize the difficulty of performing the examination well (the initial study was done by one single neuro-opthalmologist and as far as we know, no inter-reliability study has been performed with a group of generalists
- Alarming findings are useful though and should prompt further investigation
- Remember, ALL three of the following components must be seen in order to state that the exam is truly negative (and therefore a peripheral vertigo)
- Unidirectional or no nystagmus
- No vertical skew
- Abnormal head impulse test (corrective saccade) – this indicates a nerve problem and therefore must be seen in order to state that the HiNTs exam is negative and therefore the vertigo is peripheral
4. Try not to overly rely on imaging, especially a head CT, which is at best, 16% sensitive for acute ischemia in the posterior fossa. Even MRI with DWI misses 15-20% of acute posterior fossa infarctions in the first 24 hours. Sensitivity for brainstem strokes is maximal 72-100 hrs after infarction
