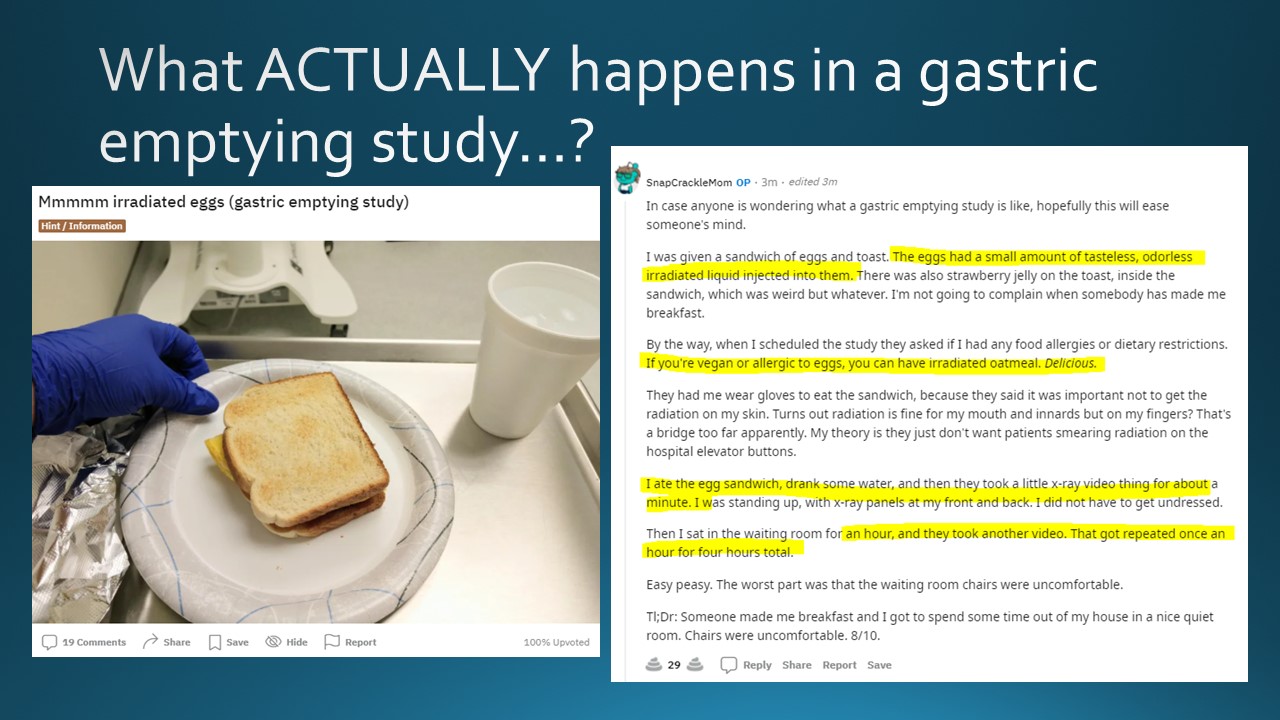
Today we discussed the case of an elderly woman with history of diabetes and afib who presented with subacute onset nausea/emesis and epigastric abdominal pain, with gastric emptying study showing marked delayed gastric emptying with >90% of food retained at 4 hours.
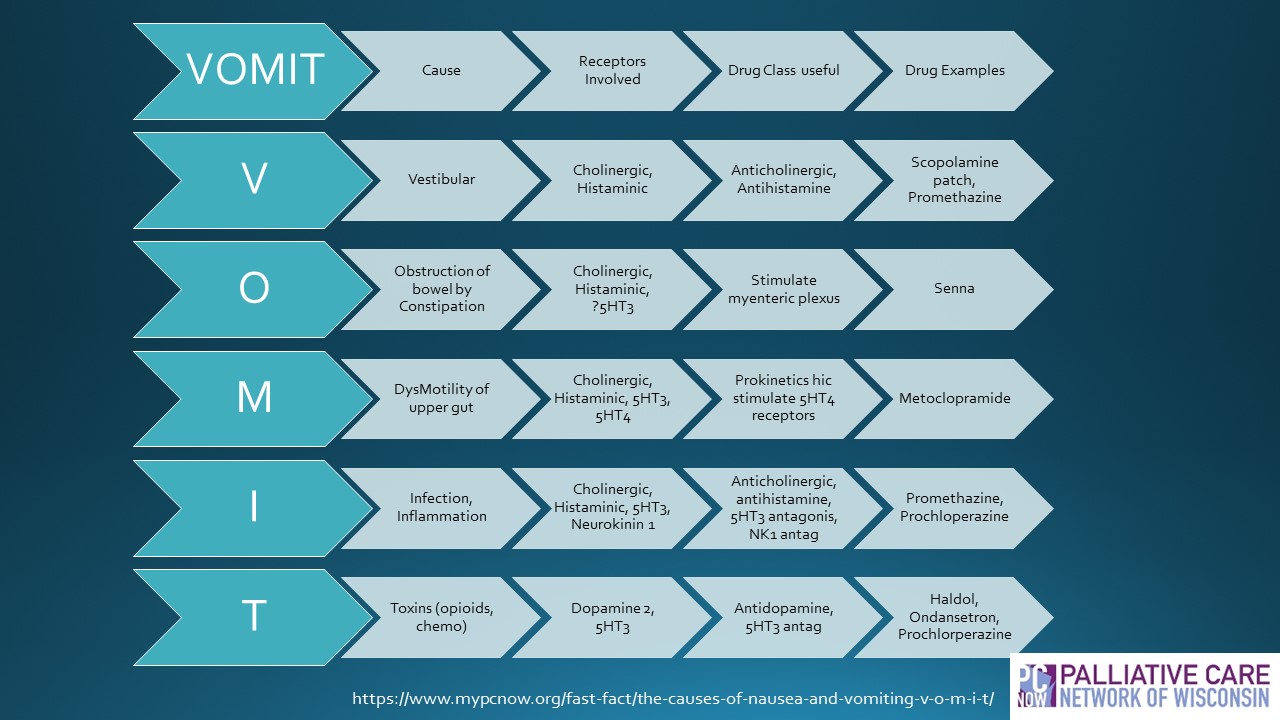
We discussed a framework for nausea/emesis as well as how to approach and treat gastroparesis.
Nausea/Emesis can be broken into Acute and Chronic etiologies.
Common etiologies for ACUTE nausea/emesis:
Infections- acute gastroenteritis
Postop Nausea/Emesis- 1/3 of surgical pts have nausea/emesis or both after general anesthesia
Vestibular Neuritis- Rapid onset severe vertigo w/ nausea/emesis, gait instability
Chemo- Common; Anticipatory antiemetic indicated when highly emetogenic chemo regimen given
Common etiologies for CHRONIC nausea/emesis:
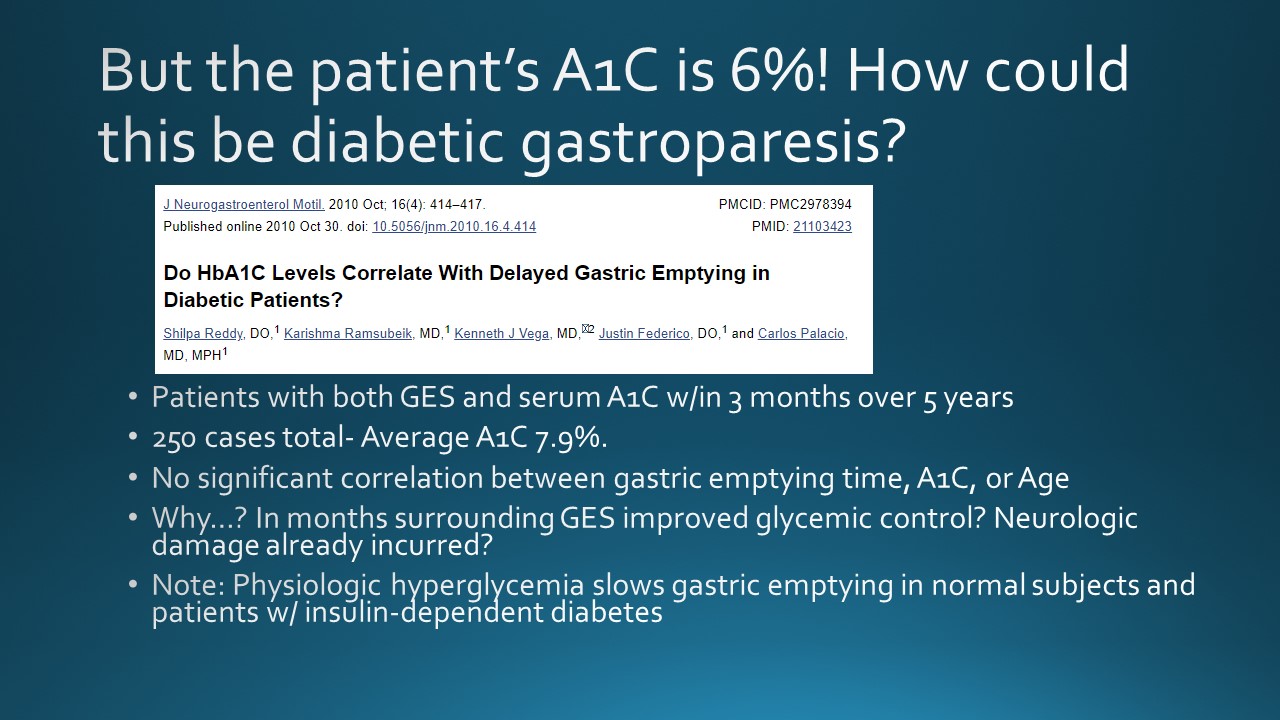
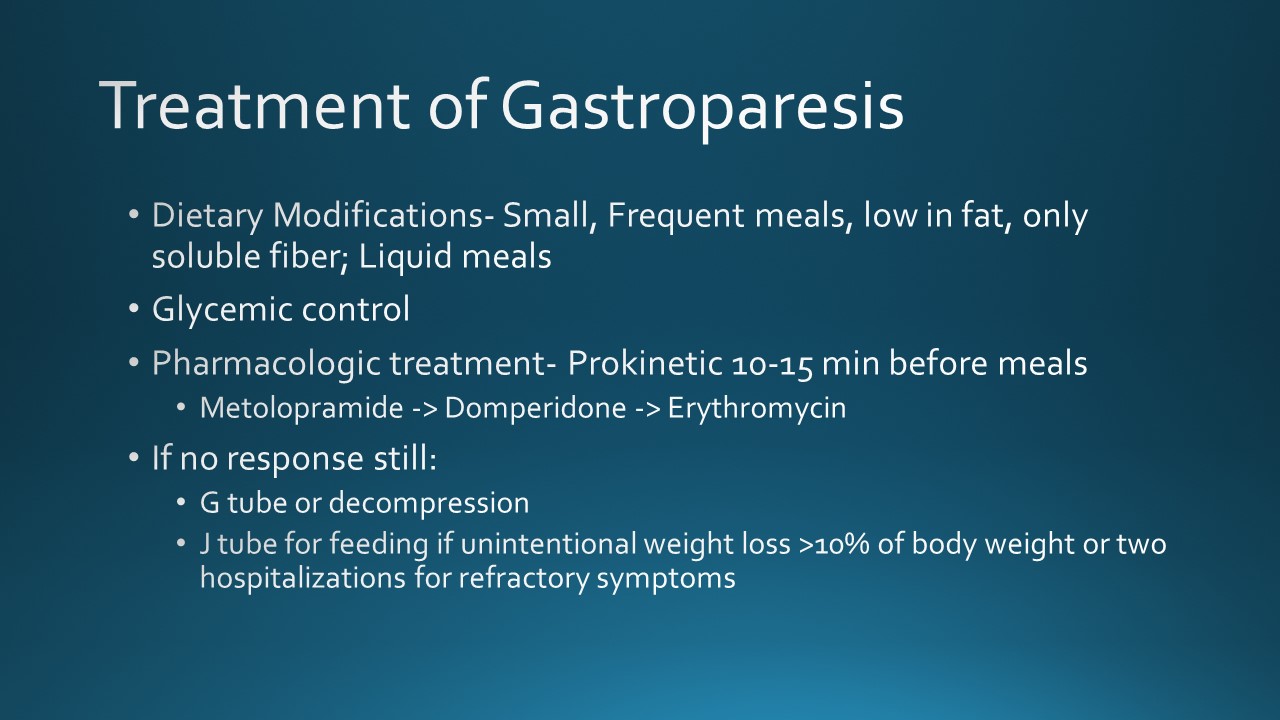
Gastroparesis – delayed gastric emptying w/o mechanical obstruction – idiopathic, diabetic
GERD
Gastric Outlet obstruction- pyloric stenosis from malignancy or PUD
Chronic idiopathic
Functional nausea/vomiting disorder