We discussed a case of a middle aged man presenting with acute onset chest pain and bradycardia in the setting of recurrent syncope. Our patient had negative troponins but ST elevations that met criteria for STEMI. STEMI alert was called, however repeat EKG did not meet STEMI criteria. Patient was admitted for unstable angina and received a stress test during which he experienced chest pain with EKG evidence of STEMI. Coronary angiogram was negative for coronary artery disease however he responded to intracardiac nitroglycerin with significant increase in the caliber of left PDA. He was diagnosed with a type of MINOCA (MI in the absence of obstructive CAD), known as vasospastic angina.
It is important to think of “do not miss” chest pain differentials using the 4:2:1 method:
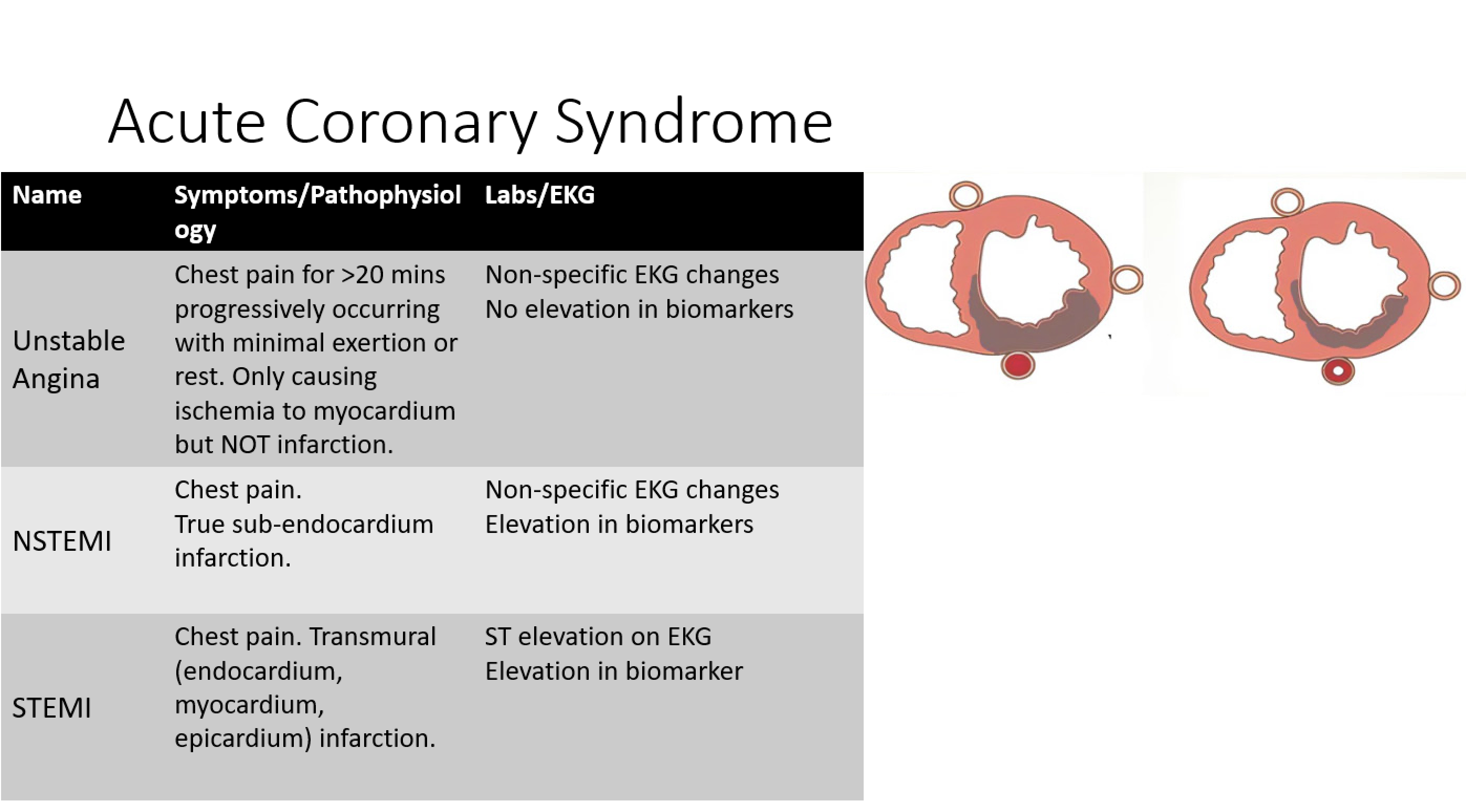
- 4 cardiac for 4 chambers – ACS, Tamponade, Aortic Dissection, Myocarditis
- 2 pulmonary for 2 lungs – Pulmonary emboli, pneumothorax
- 1 GI tract – Esophageal rupture
Our patient had a STEMI alert called however not all ST elevations equal to STEMI. It is important to know criteria for STEMI:
- ST segment elevation of >1mm at J in two contiguous leads other than leads V2-V3
- In leads V2-V3 >2mm in men older than 40yo and >2.5mm in men younger than 40 yo or >1.5mm in females