
We discussed a case about a young woman with hx of STIs (syphilis and chlamydia s/p treatment), subacute hx of migratory polyarthralgias, who presented with fevers and acute arthritis / tenosynovitis of her left index finger + thumb. She was found to have gram negative diplococci bacteremia and diagnosed with disseminated gonorrhea.
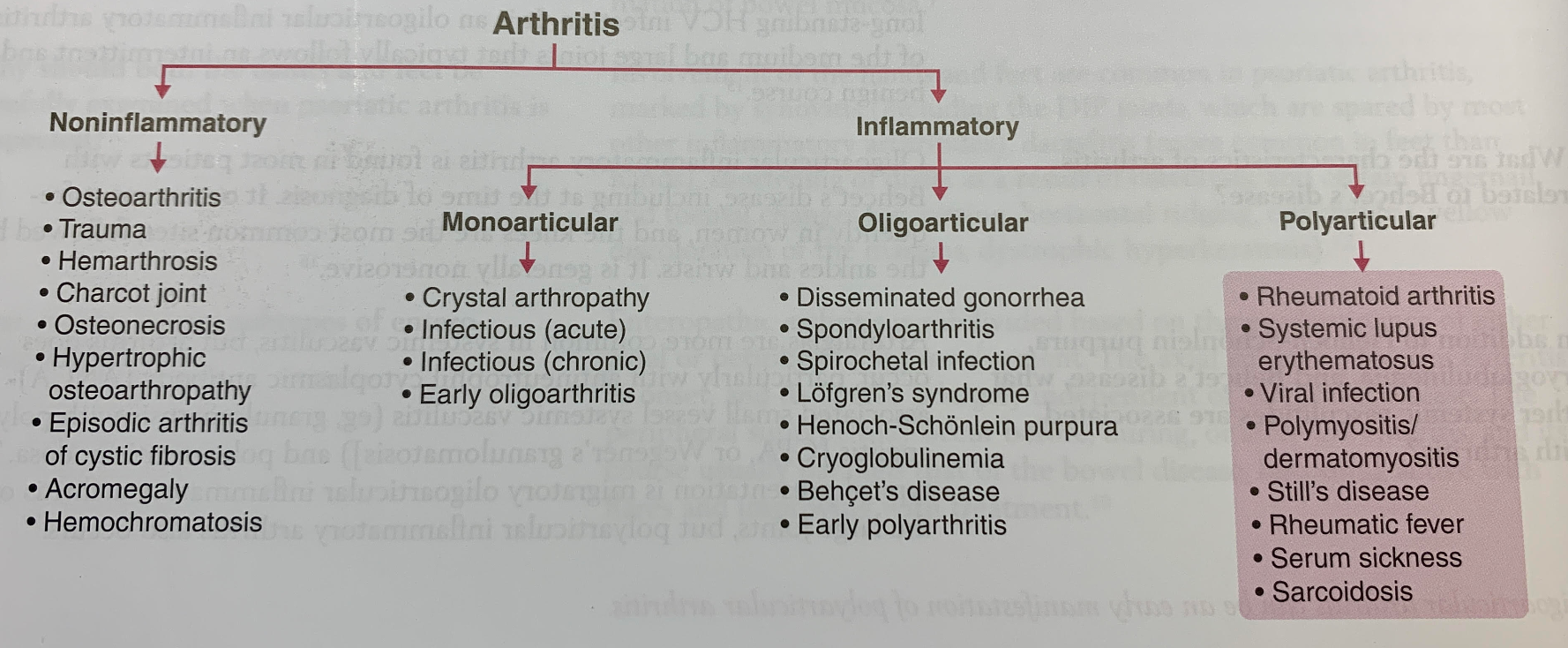
Framework for arthritis
- Categorize differentials based on non-inflammatory vs inflammatory, as well as mono- / oligo- / polyarticular.
CDC screening recommendations
- Men: those at high risk (MSM)
- Women: can be asymptomatic -> complications of STIs (eg PID, infertility)
- < 25 yrs old AND
- ≥ 25 yrs old + STI risk factors
Preferred screening / diagnostic testing
- Uncomplicated: NAAT (urine, genitals / throat / rectal swab)
- Disseminated: Blood, joint, abscess, and/or CSF cultures
Gonorrhea treatment
- CDC reports increasing azithromycin resistance
- Ceftriaxone is first line
!Bonus learning! Chlamydia treatment
- Also increasing azithromycin resistance
- Doxycycline 100mg BID x7 days is first line
